This operational playbook is for care delivery enterprise (health systems, hospitals, and ASCs) CIOs to leverage technology, particularly AI, to address four key existential challenges by their organizations: 1) revenue headwinds, 2) margin deterioration, 3) clinician shortages, and 4) patient expectations for speed, accuracy, and costs. It centers on AI as the core technology enabled by a new delivery paradigm framed by Services-as-Software™ (SaS).
Addressing these challenges with the specific steps in this playbook will yield tangible, quantifiable benefits such as increased revenue, reduced costs, improved clinician productivity, and higher patient engagement rates.
HFS Operational Playbooks are practical guides to solving key enterprise challenges that consume significant costs, time, and resources. The playbook provides enterprise leaders a realistic roadmap with specific “to-dos” to address their everyday challenges so they can clear mental and financial space to deliver next-level value.
The US healthcare delivery landscape, despite the enormity of AI-induced opportunities, is the most economically challenged industry segment. Externally driven headwinds include the One Big Beautiful Bill Act (OBBBA), which reduced Medicaid funding by close to 10% annually, slashed reimbursement rates across the board (primarily for Medicare), and a rapidly aging population with a high prevalence of chronic conditions that will continue to drive up the cost of care. Internally driven challenges include slow and low technology investments that prevent higher productivity and efficiency, unrealized benefits from M&A activities, and slow progress in finding new sources of revenue.
These challenges will manifest into four categories of threats that need immediate remediation. The rationale for urgency lies in the bleak data from the Cecil G. Sheps Center for Health Services Research at UNC, which identified 338 rural hospitals as particularly vulnerable. Other data points suggest that even urban and inner-city hospitals are vulnerable and at risk for closure.
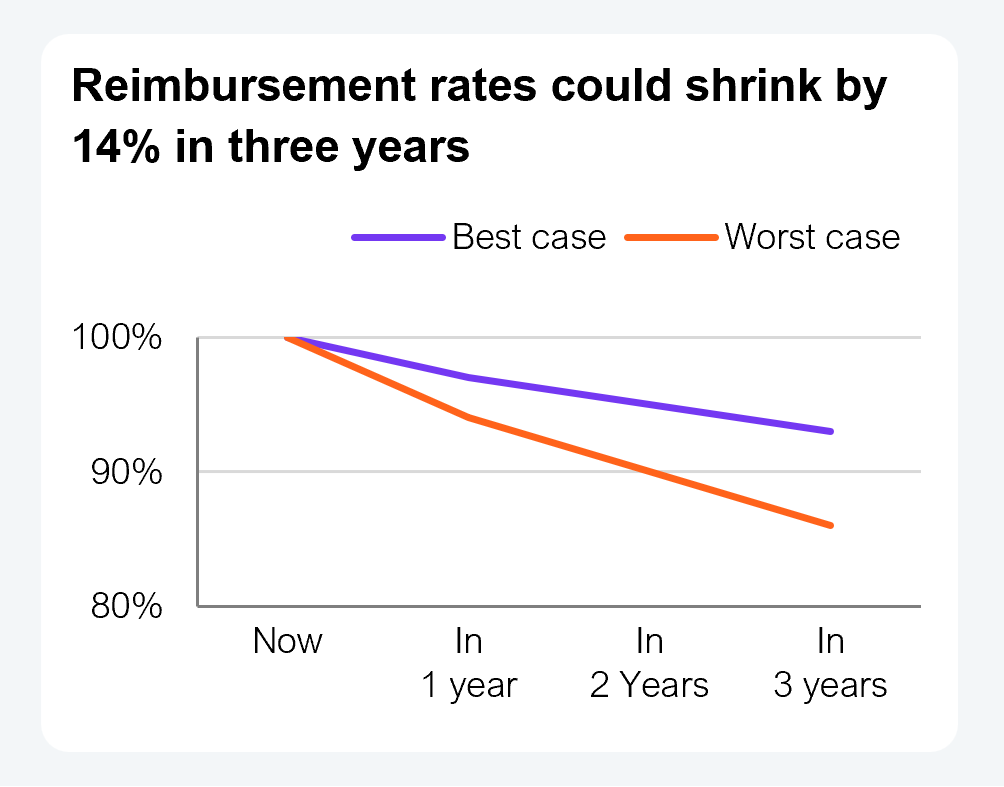
Shrinking reimbursement rates by the Centers of Medicare and Medicaid (CMS), exacerbated by site-neutral payments, increased payer friction seen in higher rates of denied or delayed payments, prior authorization, and increased uninsured rates, are reducing the number of paying patients.
These factors will reduce revenues by 3% to 6% over a 12-month period and by 7% to 14% over a three-year period for those that survive this tsunami of challenges.
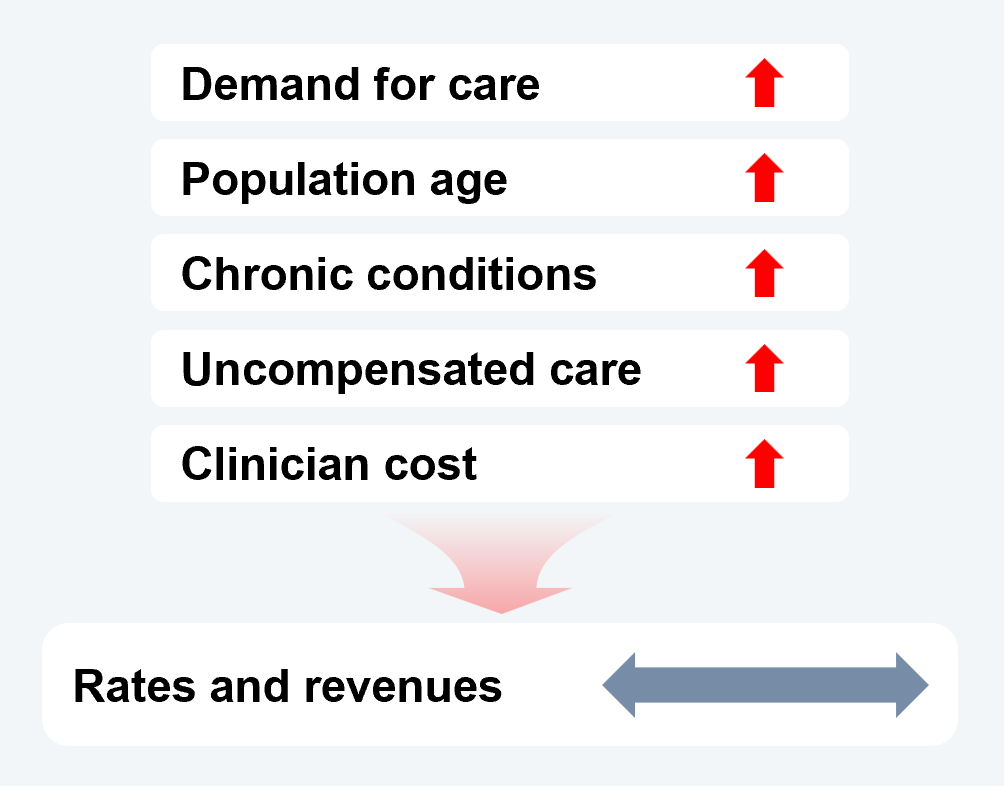
Demand for care will continue to rise as the population rapidly ages, bringing with it an increased prevalence of chronic conditions. Yet there will not be a commensurate increase in rates or revenues.
Increased uninsurance will triple the rate of uncompensated care, while the cost to attract and retain clinicians will grow only at rates above nominal inflation. Healthcare does not have a demand problem, just a monetization problem.
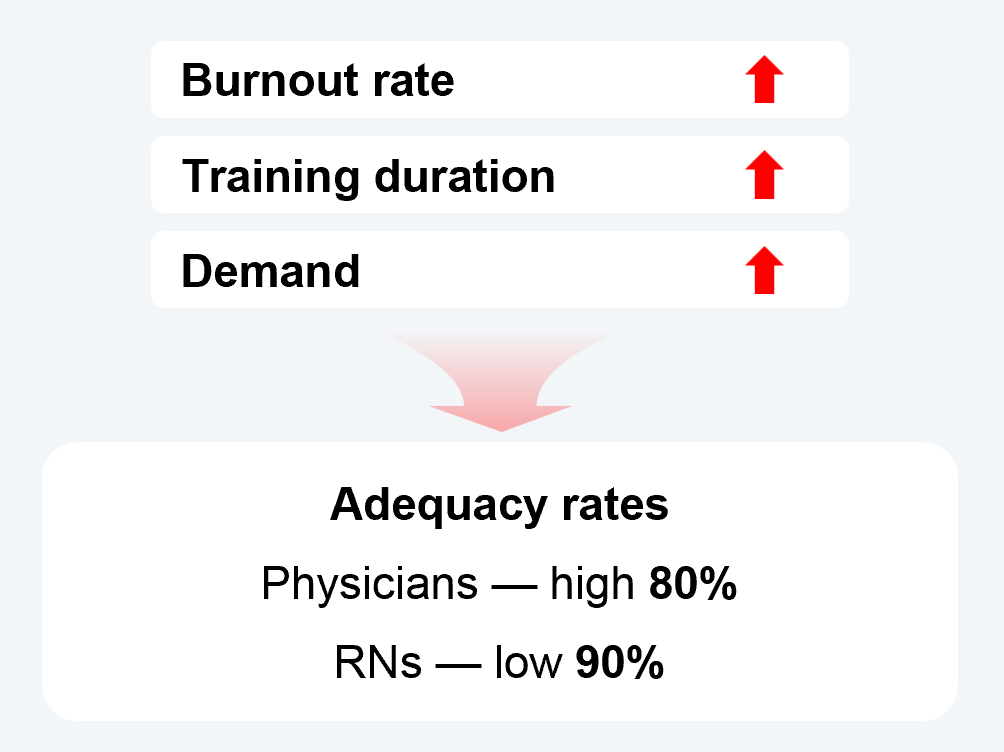
Burnout rates, slow speed to train replacements, and increasing demand for care are just some of the reasons clinician adequacy rates are likely to be in the high 80% range for physicians and in the low 90% range for registered nurses.
That rate will be worse for specialties most needed by the population based on demographics, such as primary care, geriatric care, and cardiology.
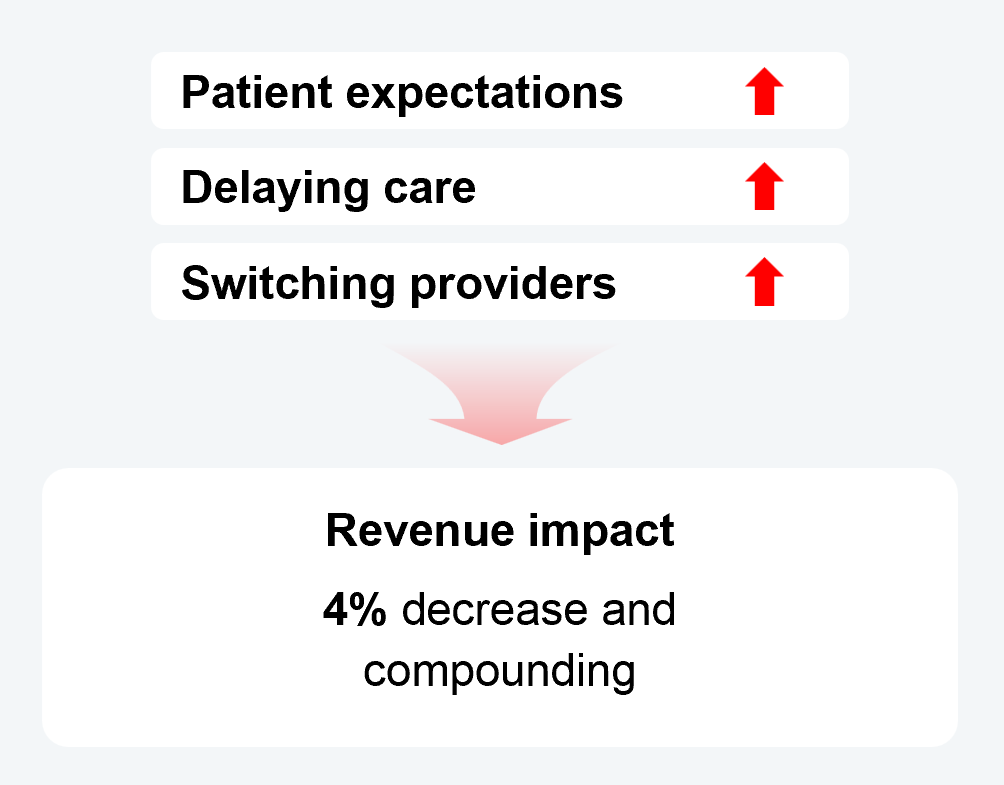
Despite rising uninsurance rates, consumers remain primarily in control of who they see for care and when. In that context, their evolving expectations for speed, accuracy, and cost are critical to understand and address. The Kaiser Family Foundation reported that 36% of adults in the past 12 months have skipped or postponed care they needed because of cost. Other data indicate that up to 50% of consumers will switch doctors if their expectations are not met.
These factors can cost as much as 4% of annual revenue over 12 months and will compound if left unaddressed.
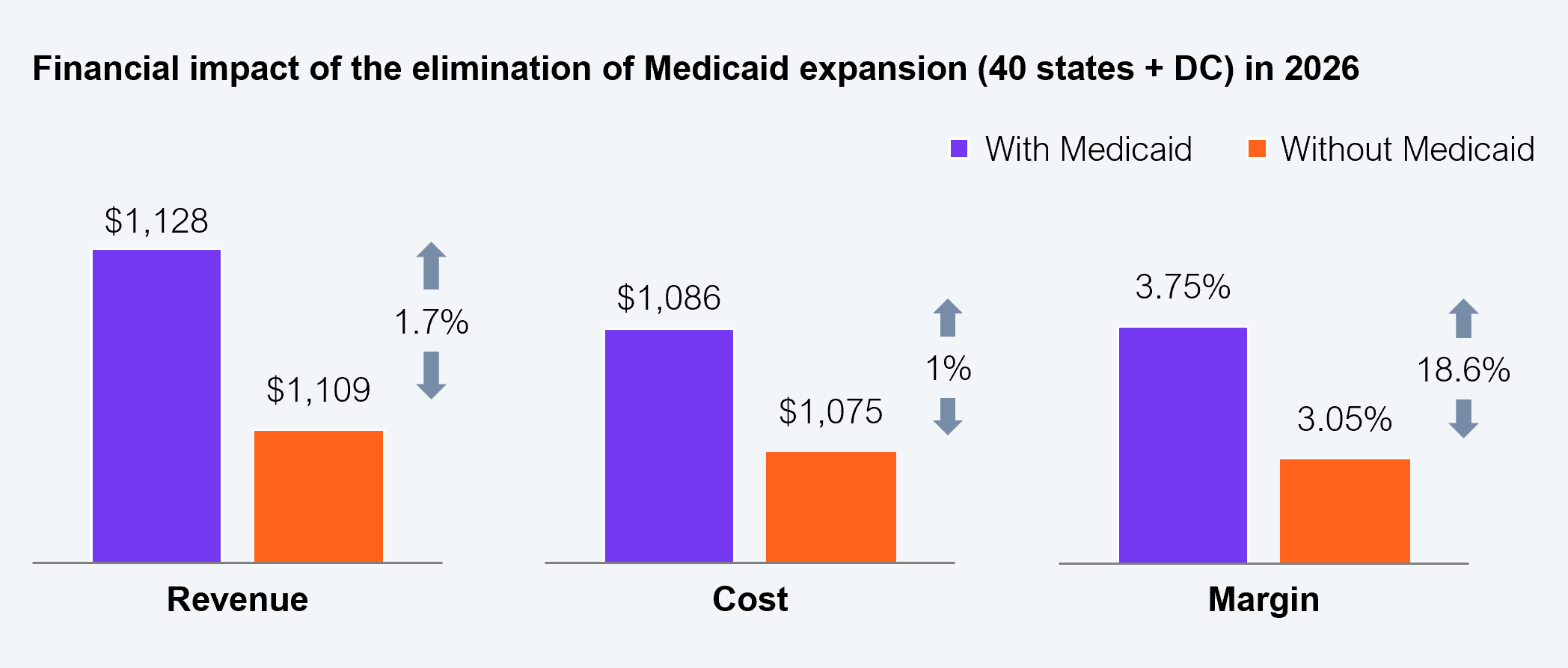
Source: Urban Institute, Commonwealth Fund, HFS Research, 2026
Health system CIOs must lean into the business of care delivery. This playbook takes a programmatic approach, enabling CIOs to execute a strategic roadmap with contained solutions that optimize their existing assets while allowing AI to deliver significant business benefits in quick succession.
Care delivery CIOs must feel comfortable with an AI-enabled, modular approach to addressing the four key business challenges, rather than relying on legacy platform enablement. Modularity will not preclude tight integration; however, that integration must be considered notional by adopting Services-as-Software™ (SaS) as the delivery paradigm (see Exhibit 2).
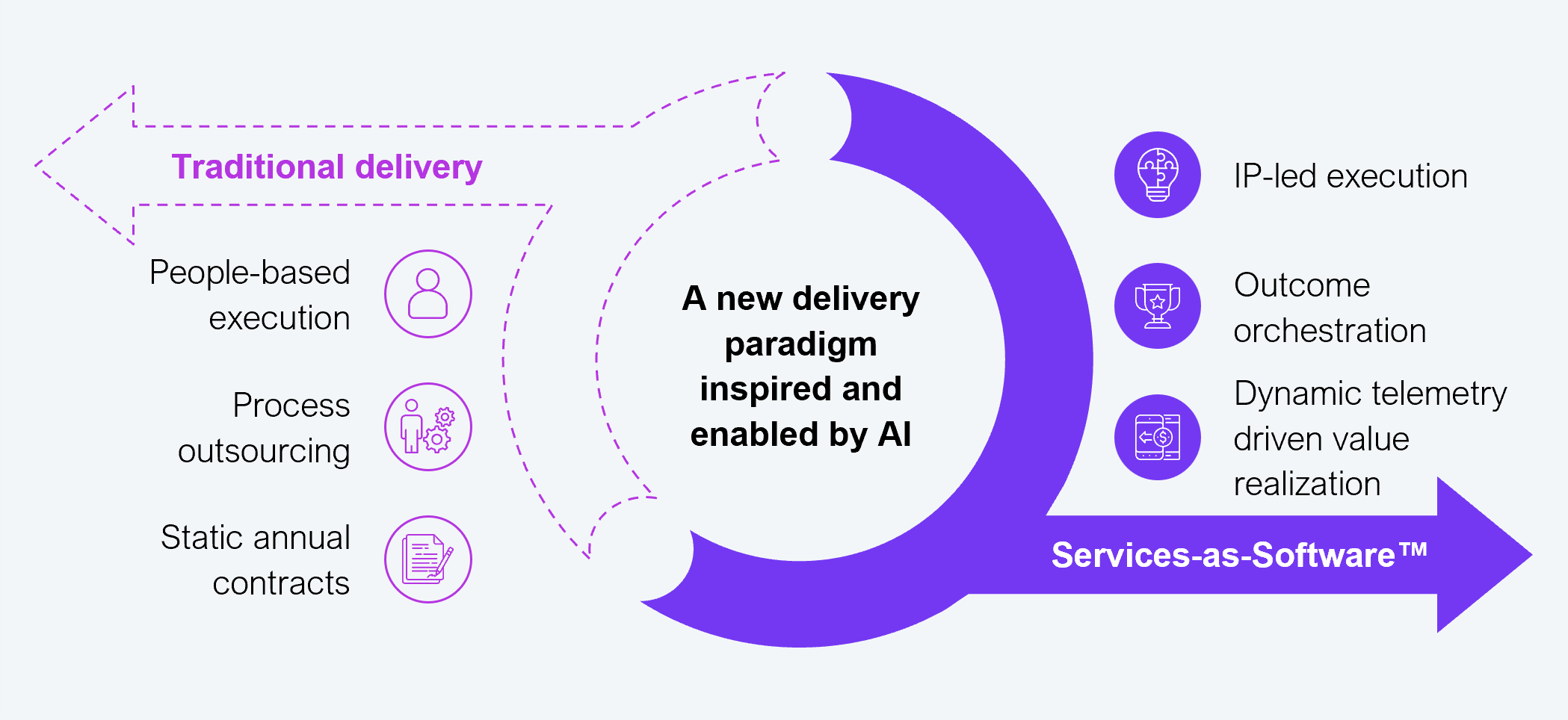
Source: HFS Research, 2026
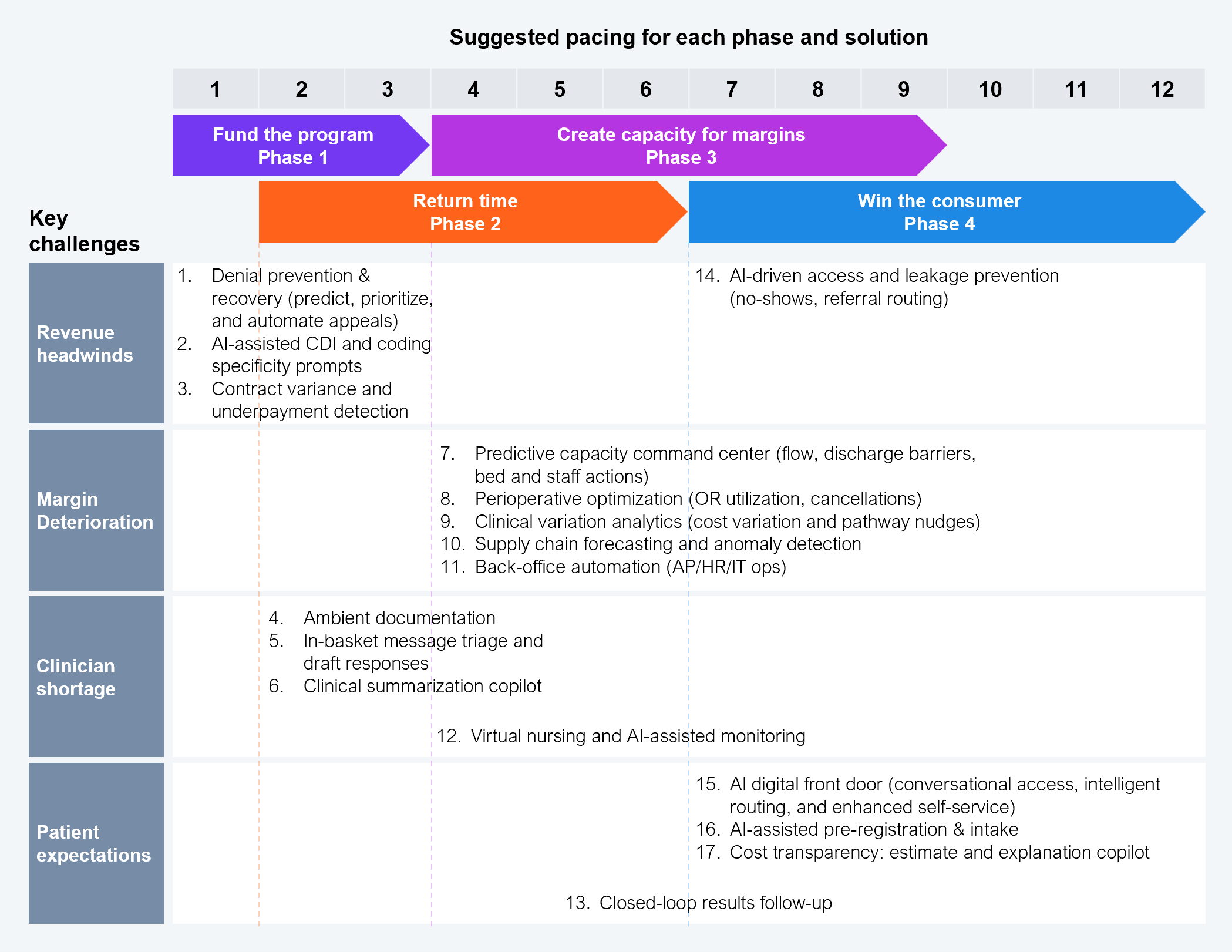
This playbook has identified 17 key solutions for delivering the largest bang for the buck in the least amount of time, leveraging existing tech-enabled capabilities and adopting SaS to deliver (see Exhibit 3). These solutions have been laid out in a practical sequence that will allow CIOs to achieve rapid ROI with lower risk, easier governance, and avoid the typical challenges of being stuck in pilot purgatory.
Source: HFS Research, 2026
This playbook has been developed with inputs from tens of practitioners, technologists, and healthcare experts. The intent is to rapidly deliver 17 solutions across four phases to directly address financial headwinds, margin deterioration, clinician shortage, and patient expectations.
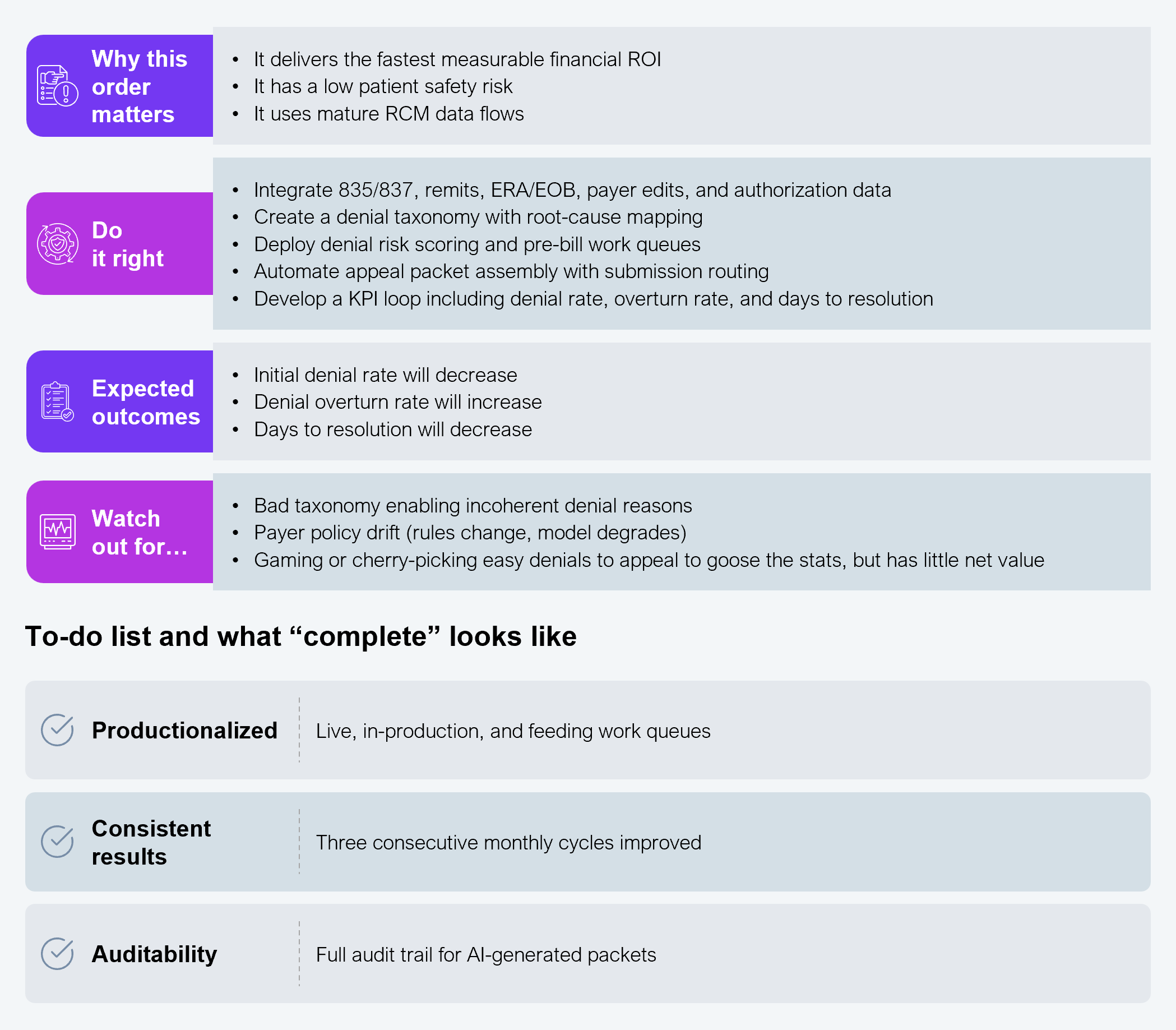
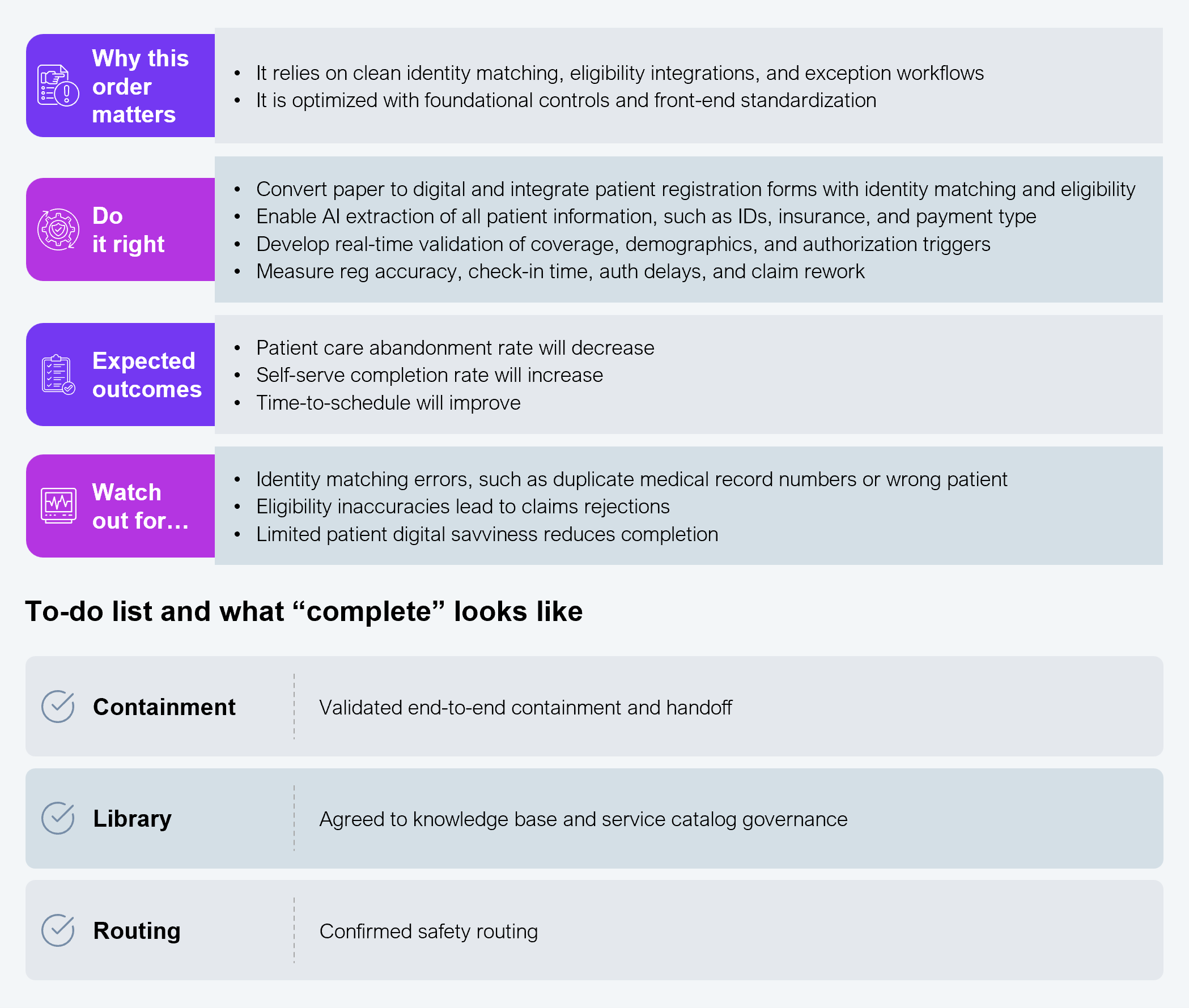
Phase 1 addresses revenue headwinds. These four solutions fund the overall program and mitigate the need for capital expense or net new investments. You must implement three of these solutions in Phase 1; you can implement the fourth in Phase 4.
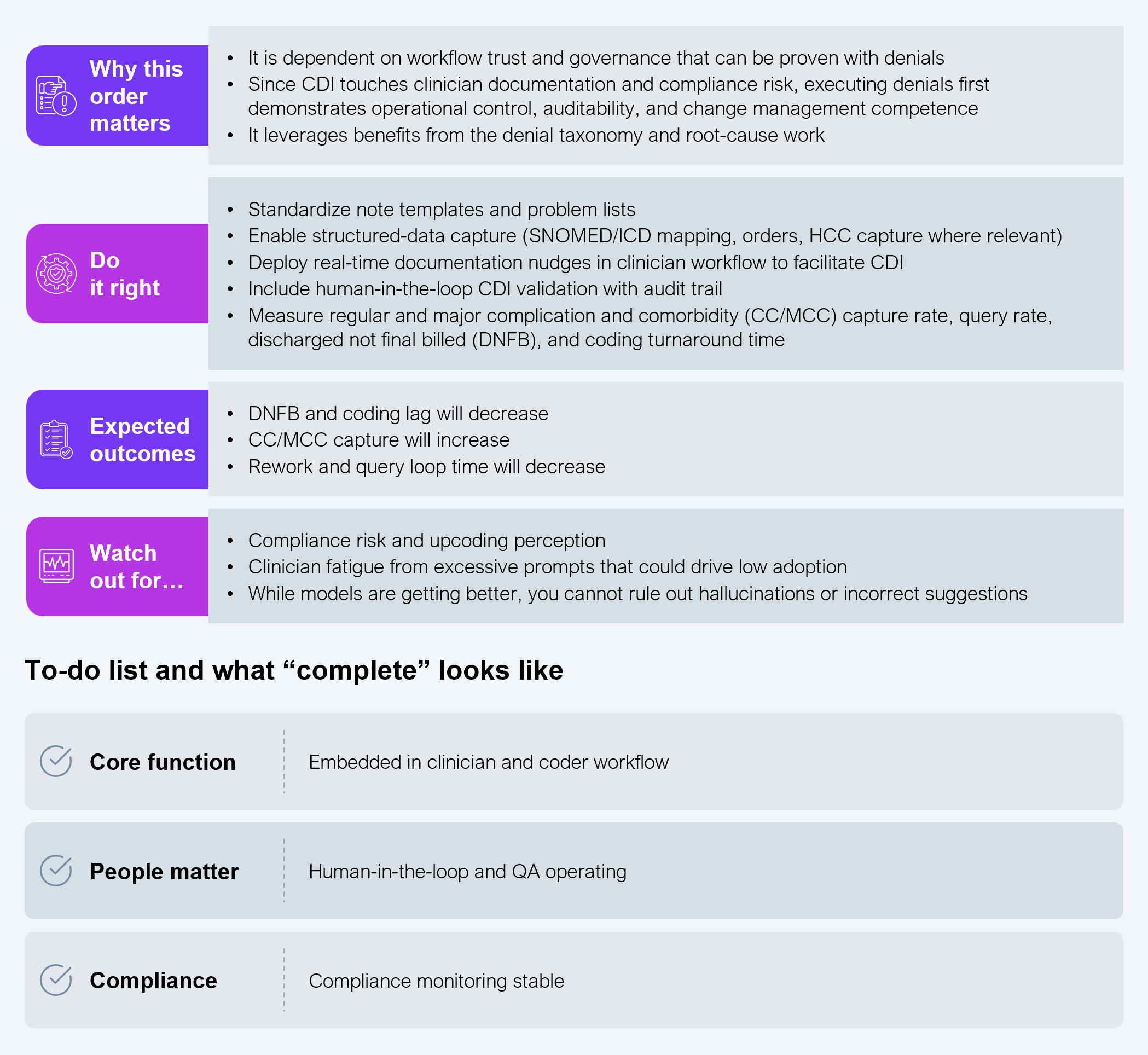
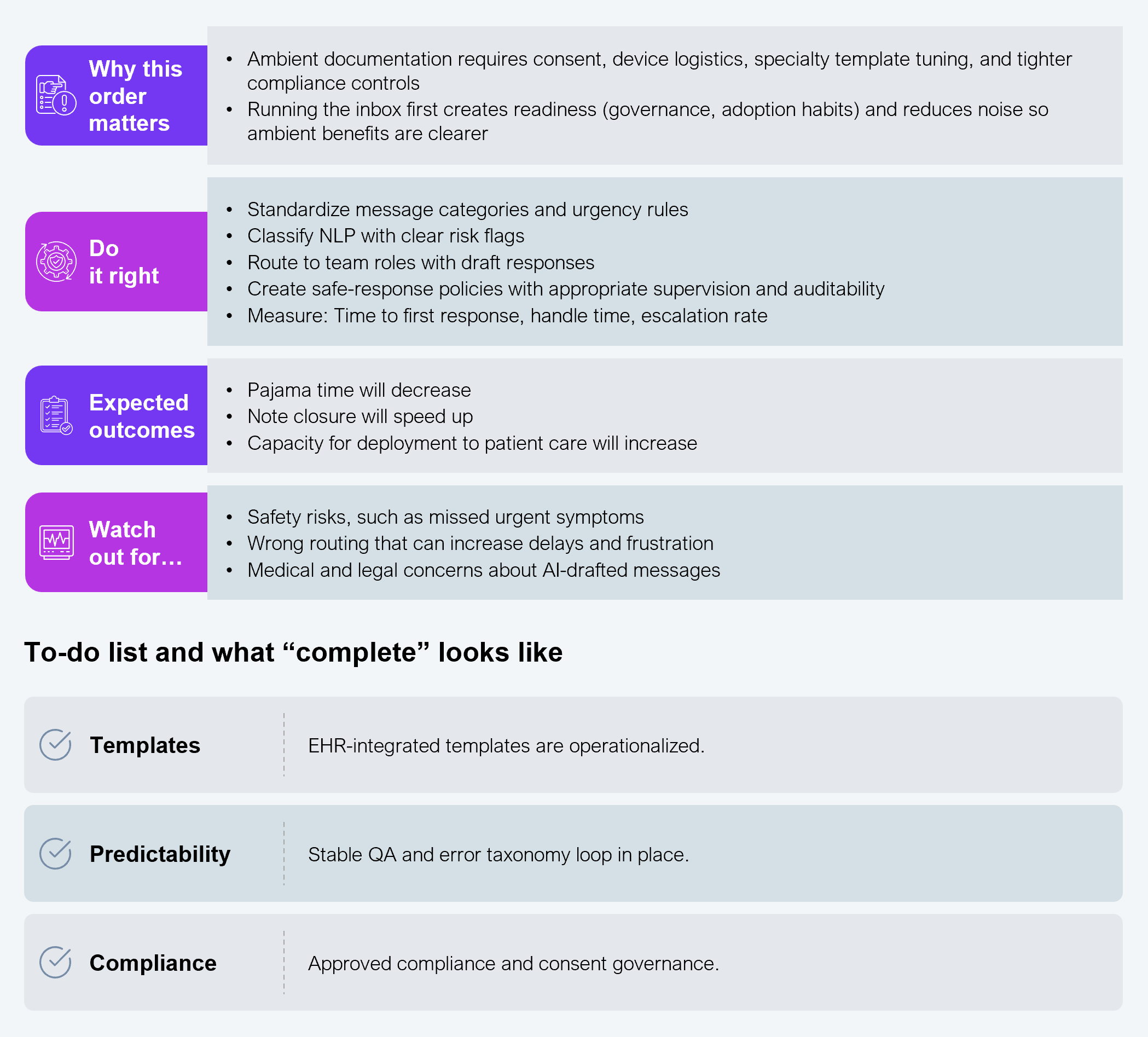
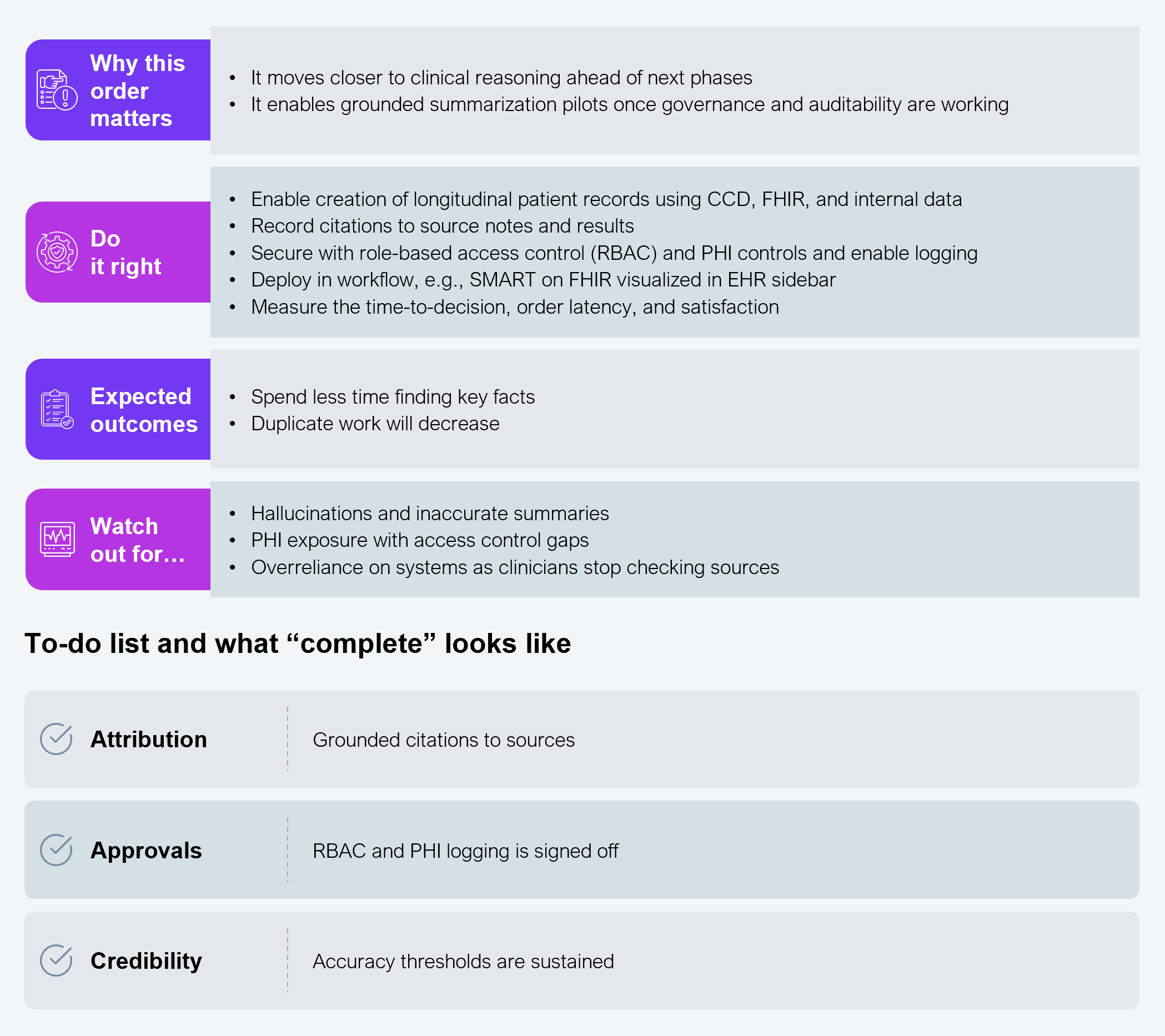
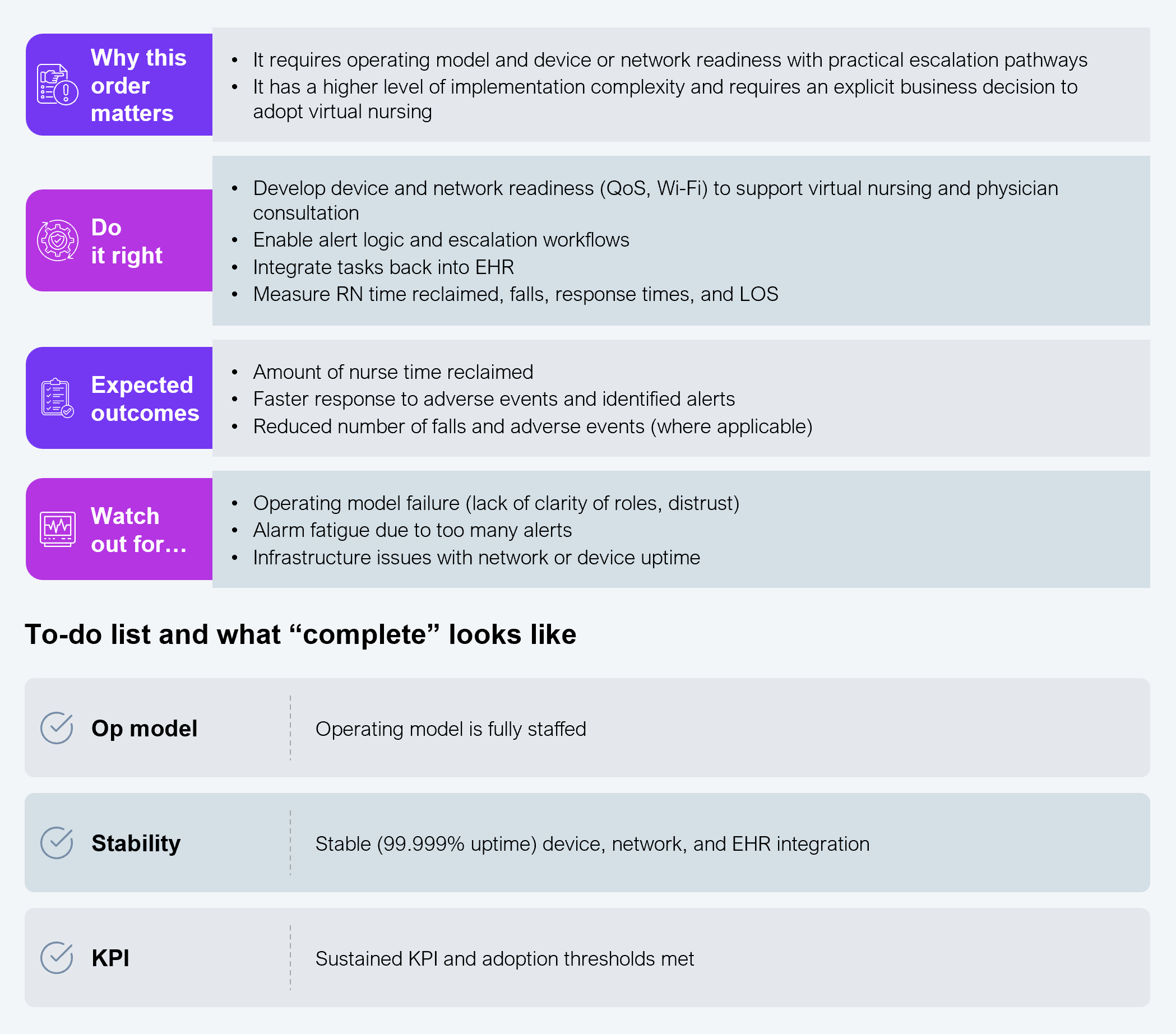
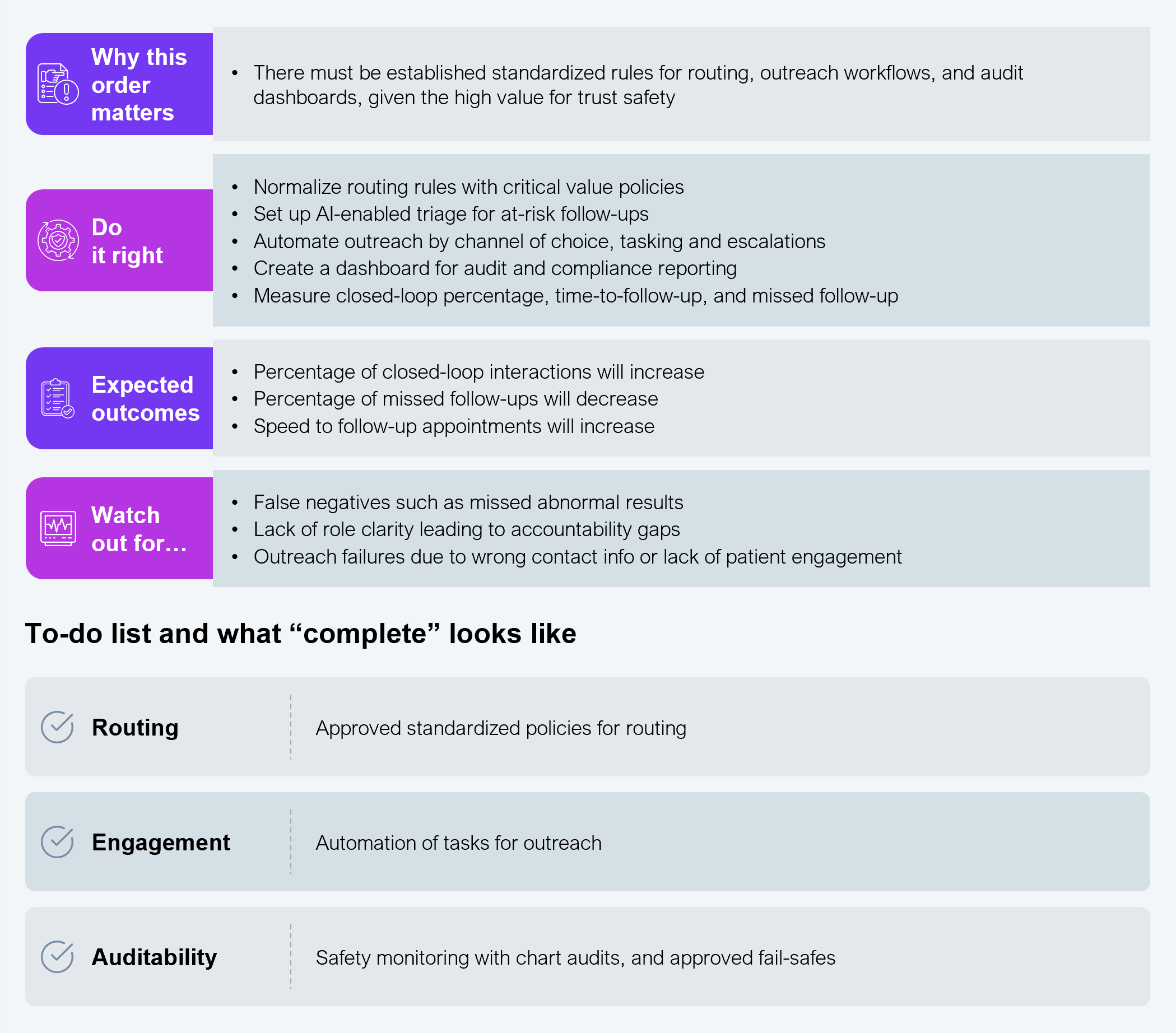
Given the shortage of clinicians, the idea is to optimize clinician time by returning time to them with these four solutions. We recommend executing the first three in Phase 2 and the fourth in Phase 3.
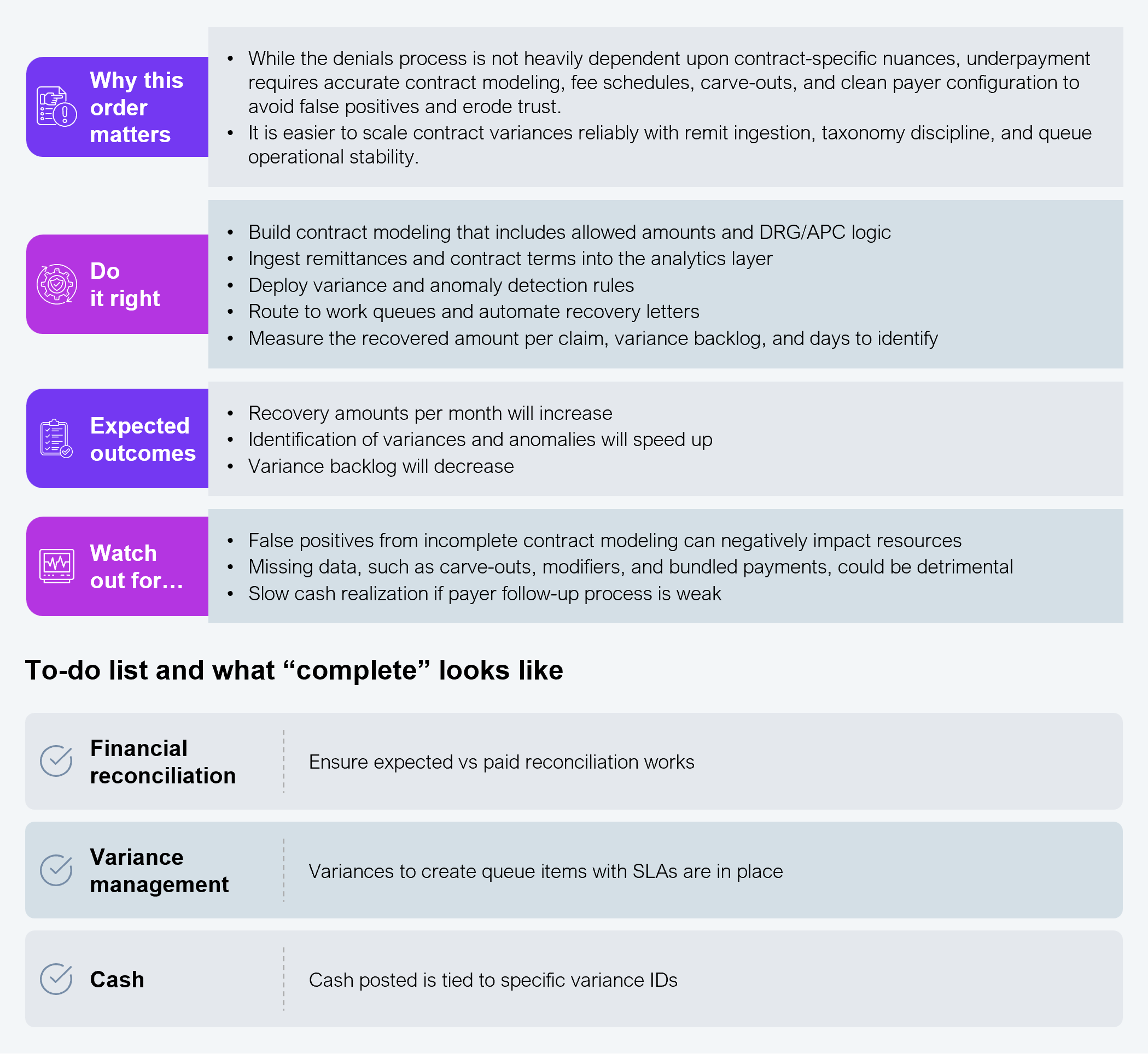
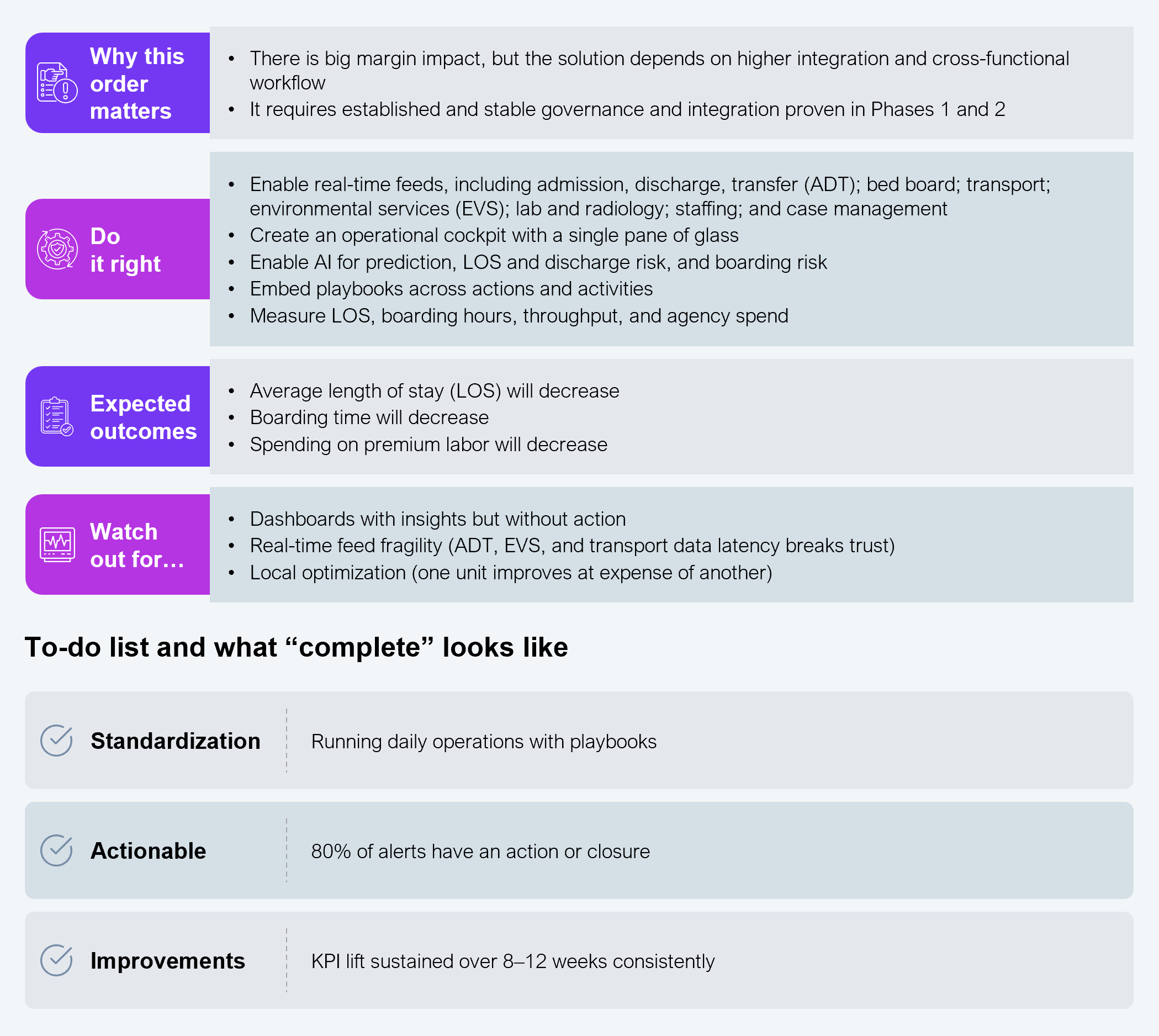
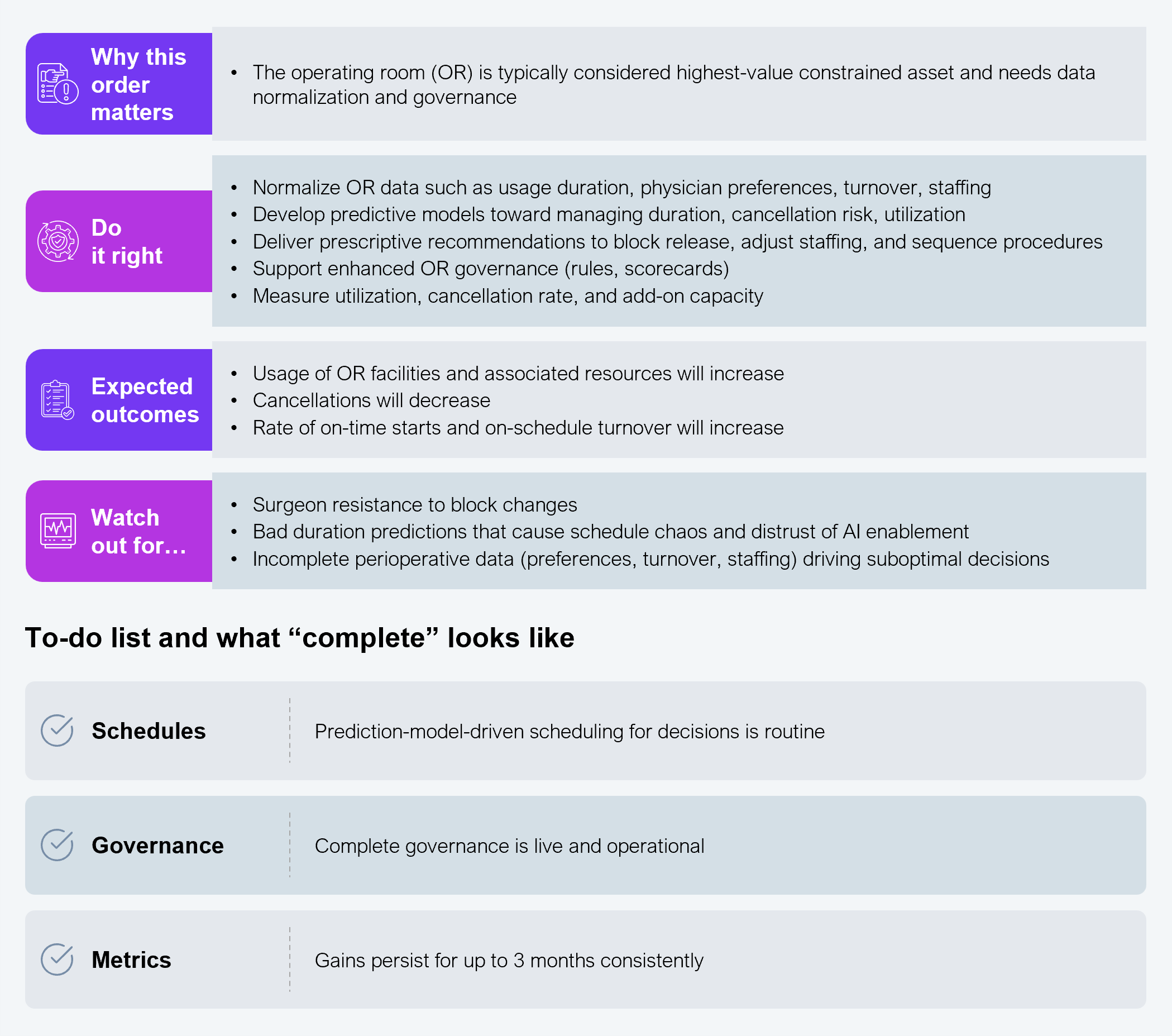
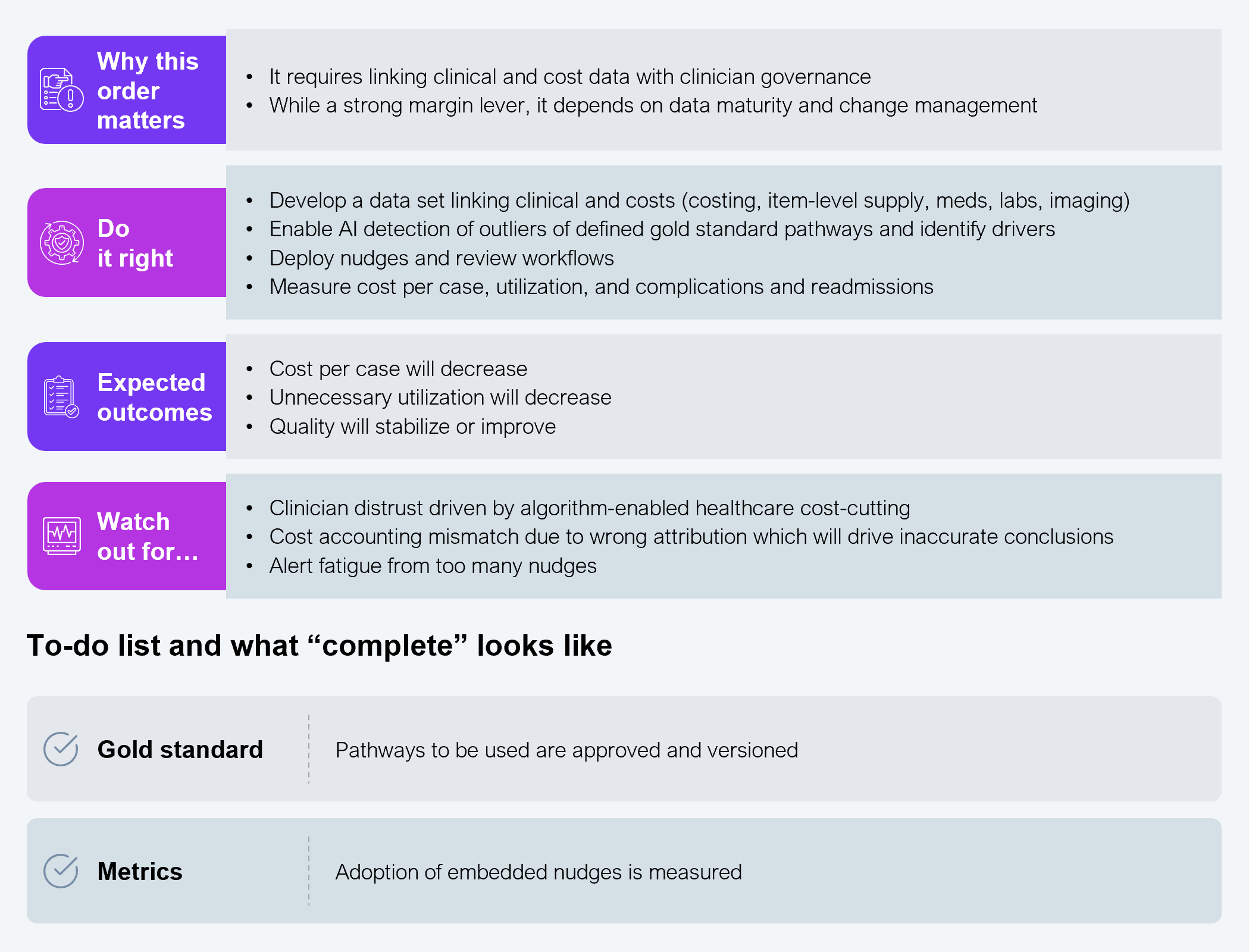
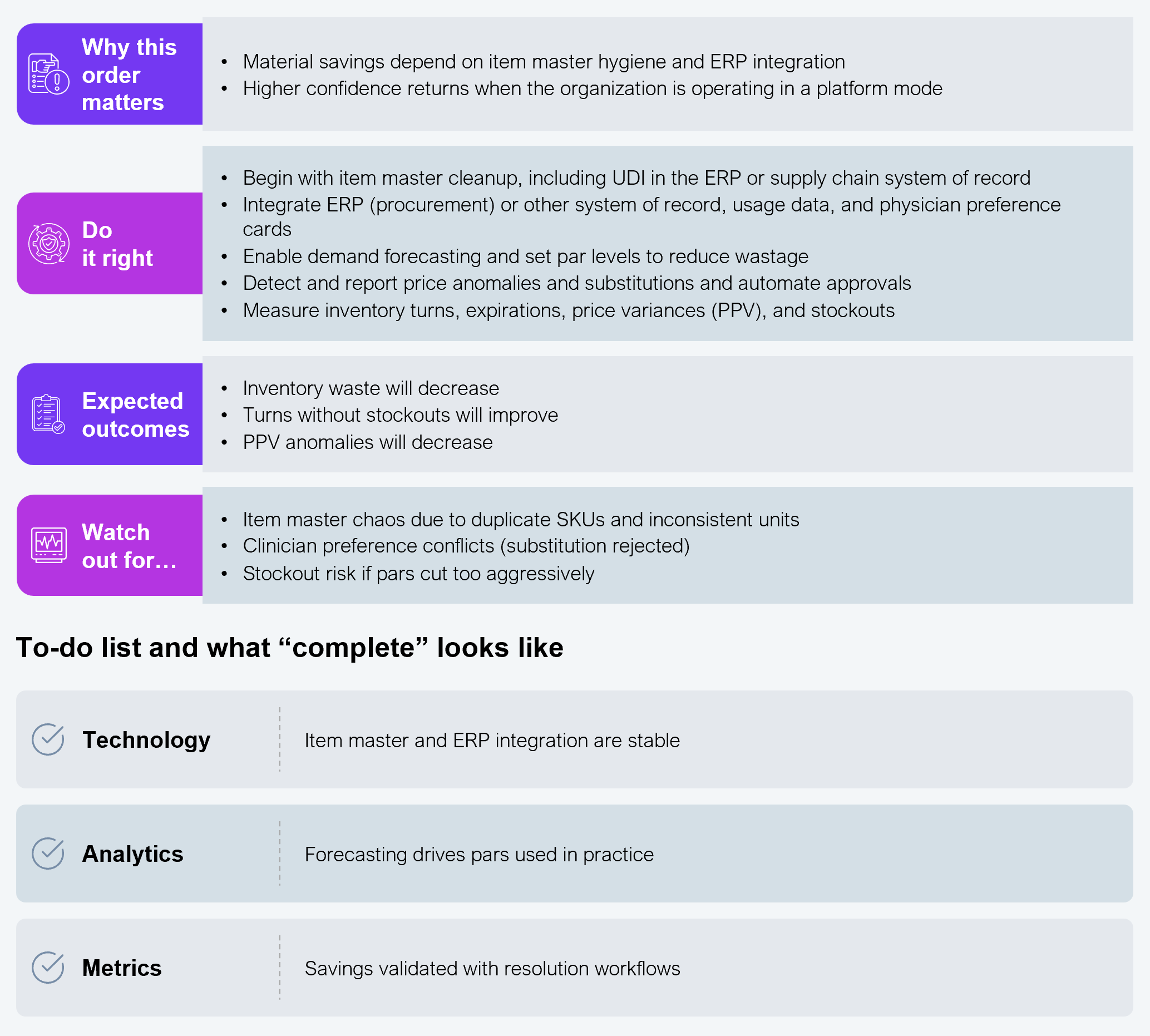
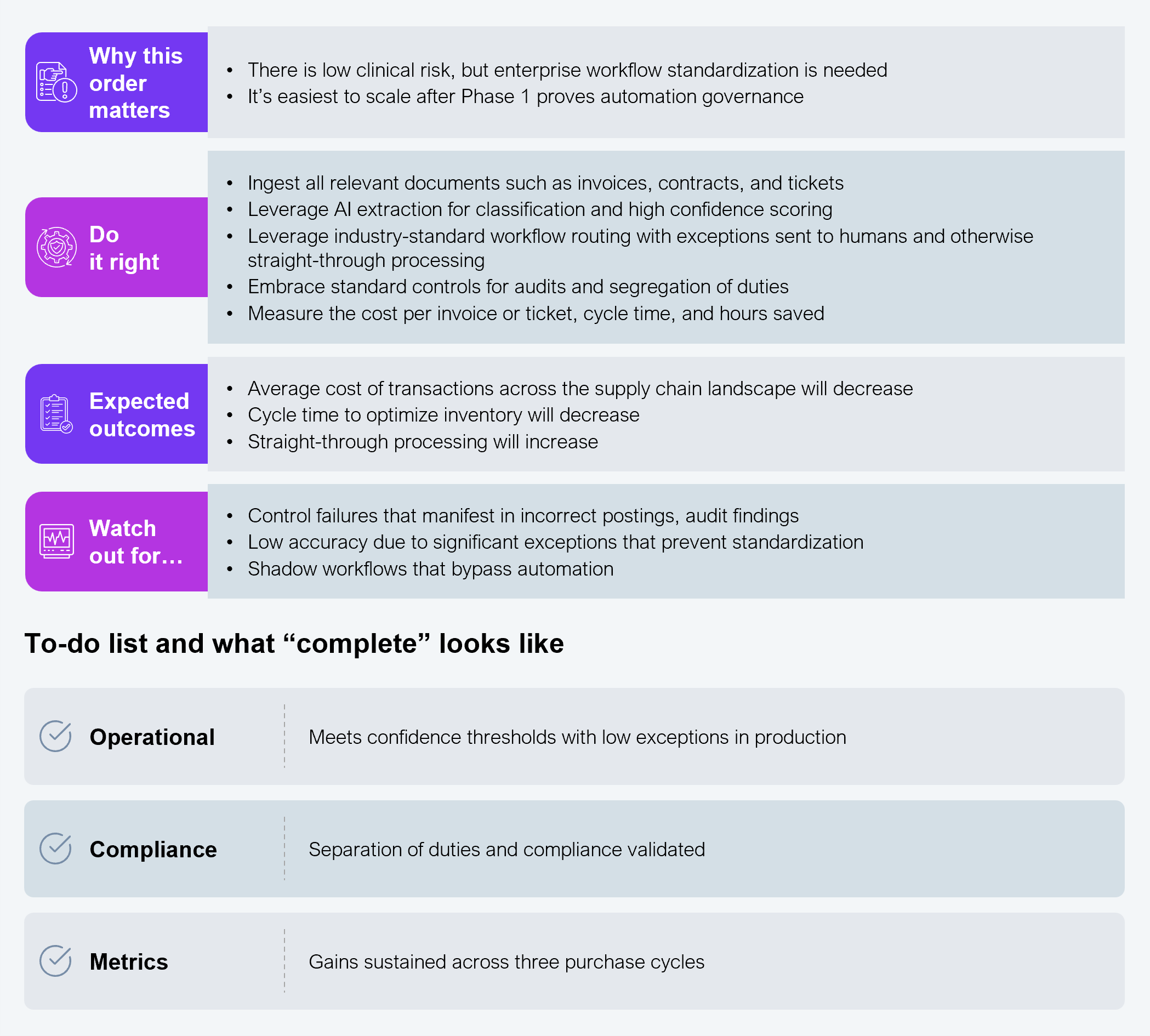
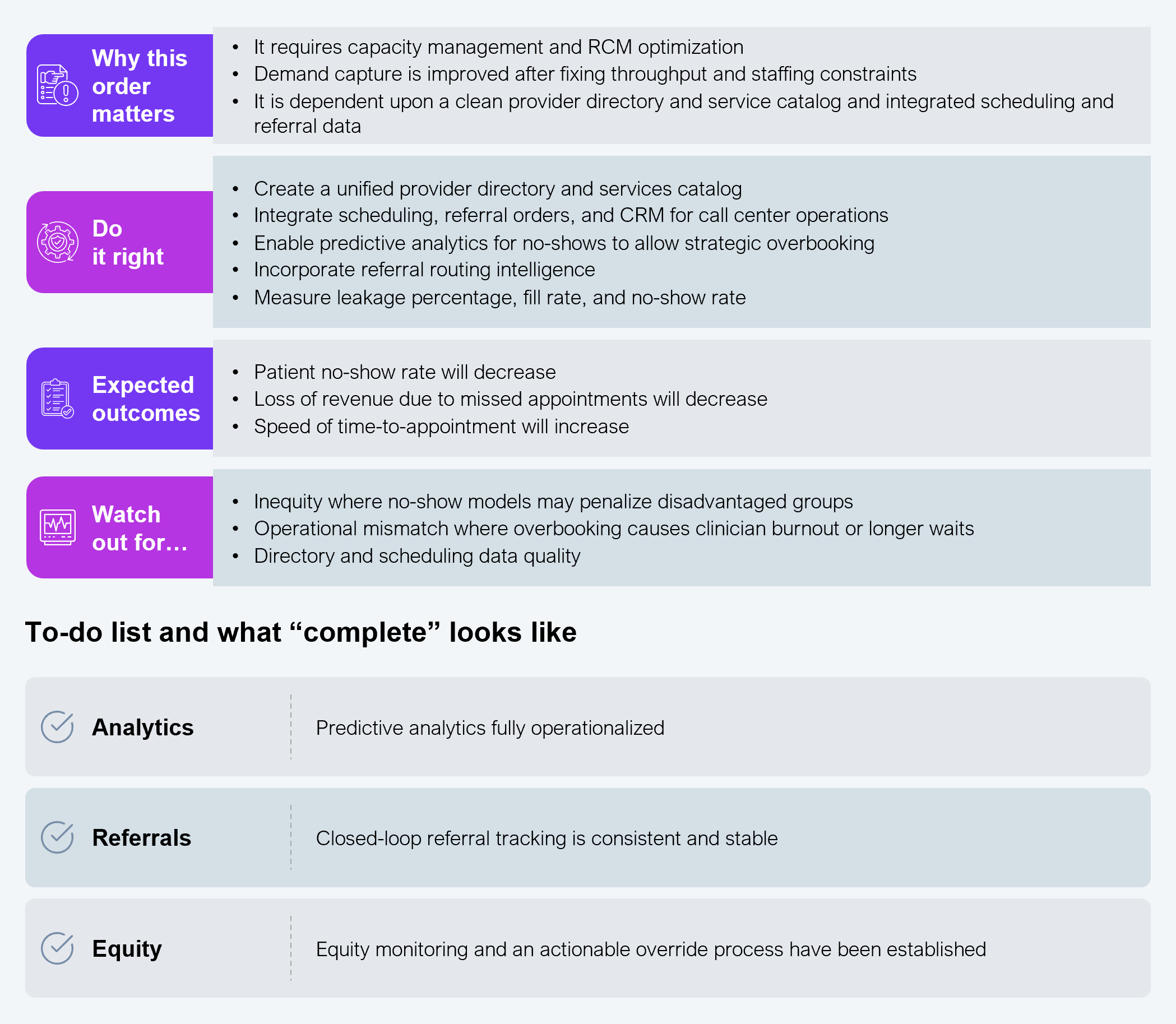
Phase 3 addresses margin deterioration with seven solutions.
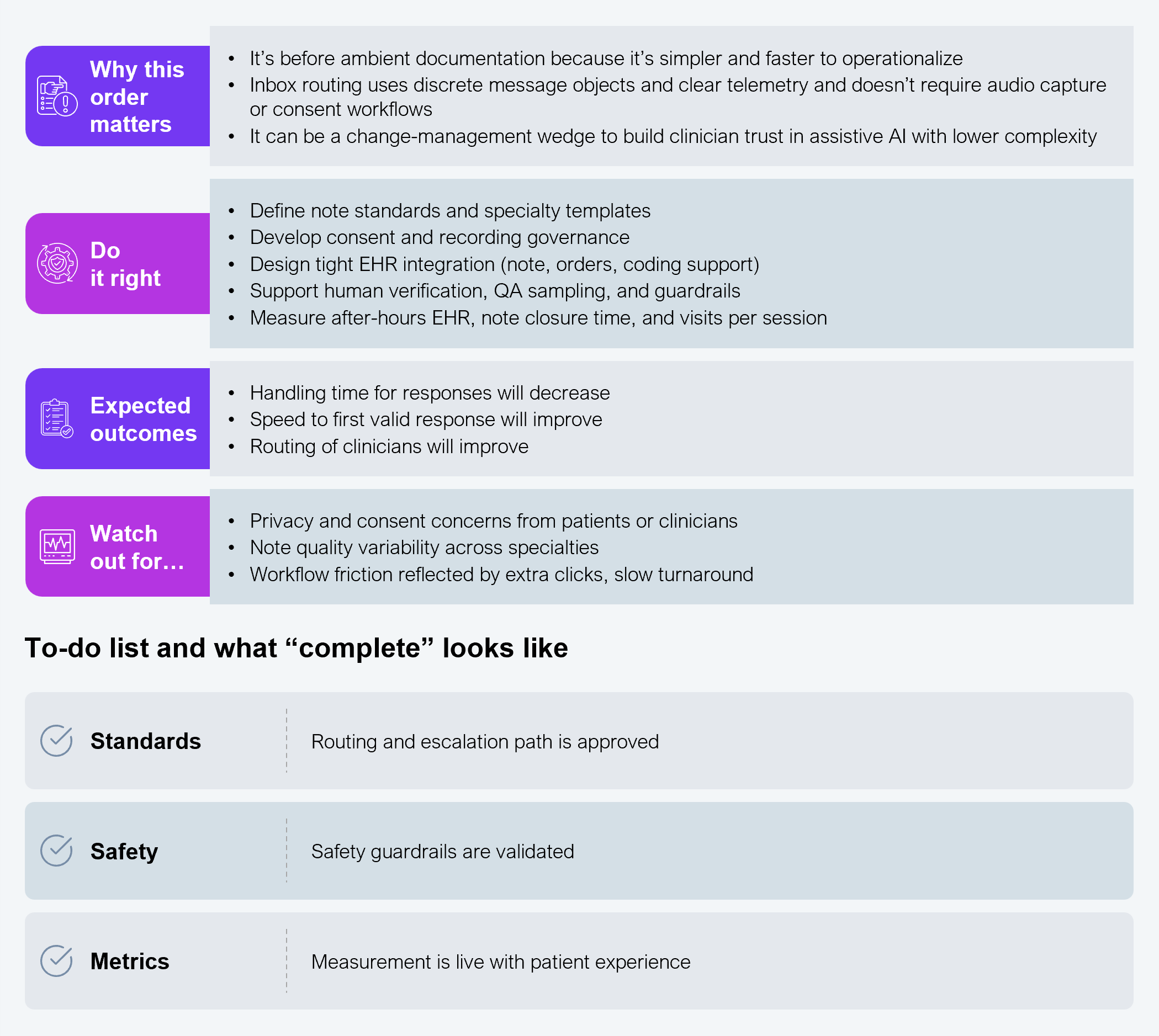
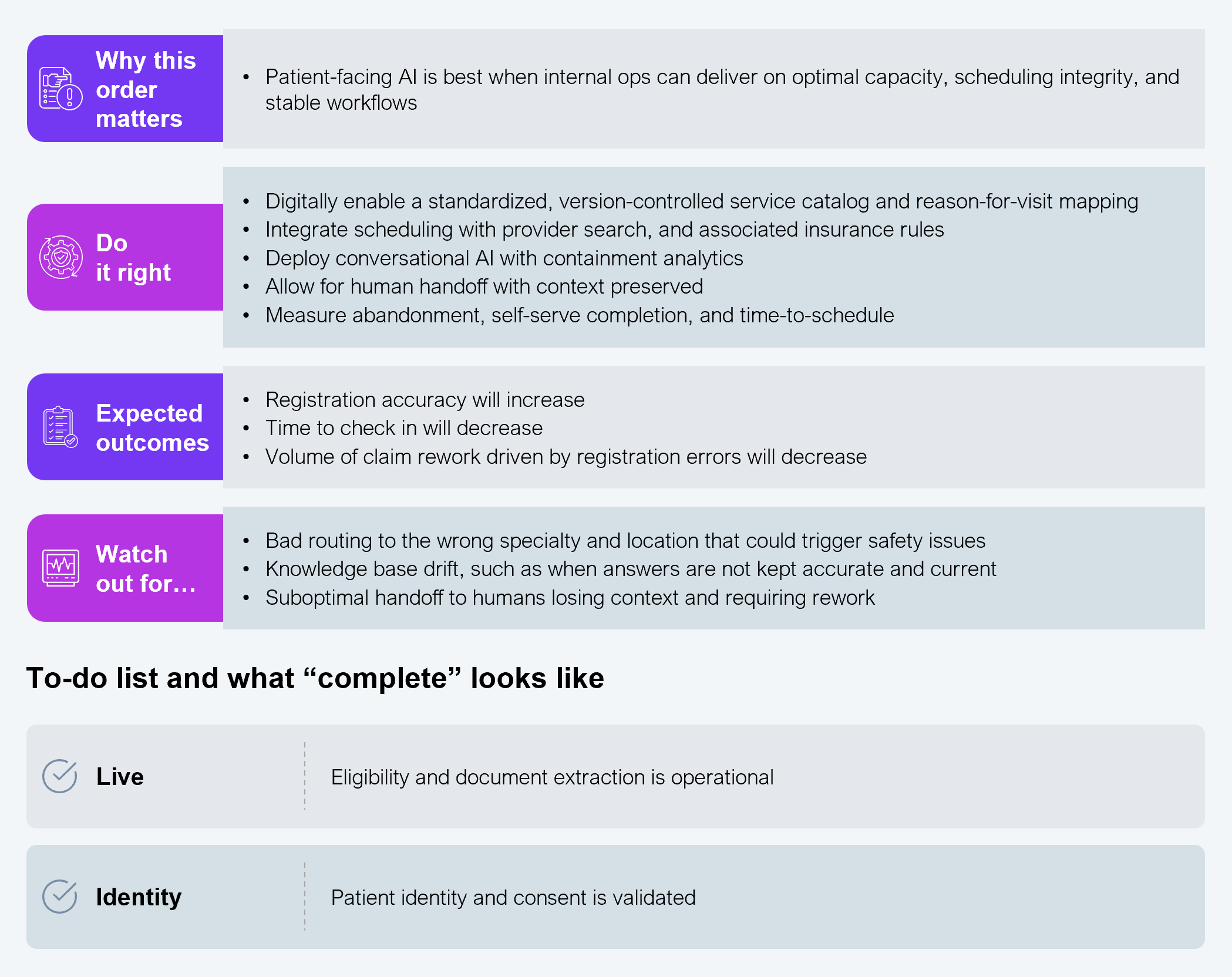
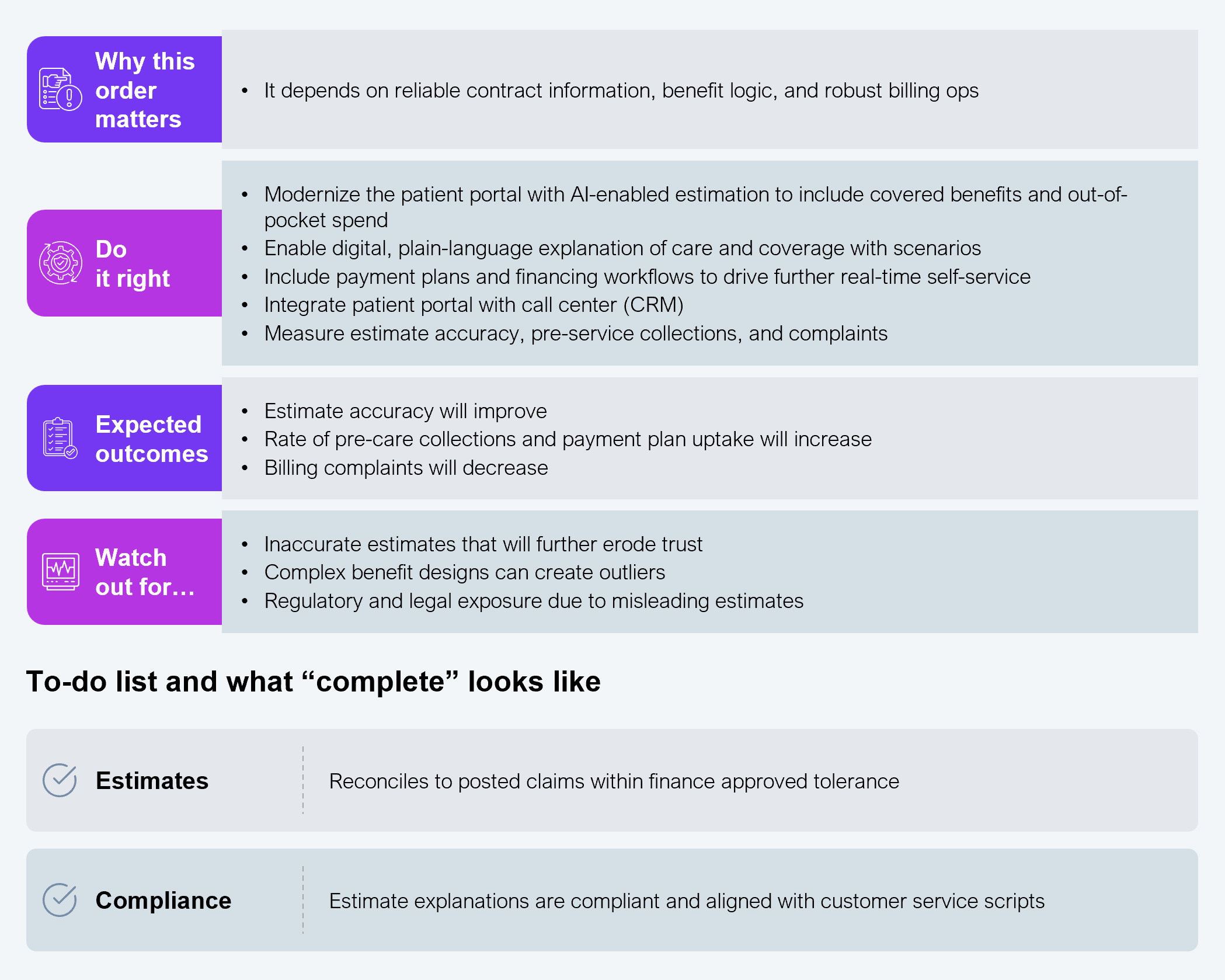
Patients’ evolving expectations are biased toward increased digital tool usage. We recommend these four solutions to address patients’ needs for faster care, higher diagnostic accuracy, and lower costs.
The following list includes relevant HFS perspectives on care delivery operations in a shifting market; watch for our series on executing Services-as-Software within a health plan and on selecting the right partner for success.
If you don't have an account, Register here |
With the exception of our Horizons reports, most of our research is available for free on our website. Sign up for a free account and start realizing the power of insights now.
Our premium subscription gives enterprise clients access to our complete library of proprietary research, direct access to our industry analysts, and other benefits.
Contact us at [email protected] for more information on premium access.