This HFS Operational Playbook is for CIOs of US health plans using AI to manage population risk, improve medical loss ratio, and protect margins.
This playbook is for CIOs of US health plans who must enable the technologies, data infrastructure, and AI capabilities required to improve medical cost performance while supporting provider and member experience. It helps them embrace the key tenets of Services-as-Software™ and leverage AI to reduce costs and operational risks.
When executed with discipline, this approach enables health plans to materially reduce avoidable hospitalizations, improve chronic condition control, and bend the medical cost curve while preserving compliance and risk posture.
HFS Operational Playbooks are practical guides to solving key enterprise challenges that consume significant costs, time, and resources. The playbook provides enterprise leaders a realistic roadmap with specific “to-dos” to address their everyday challenges so they can clear mental and financial space to deliver next-level value.
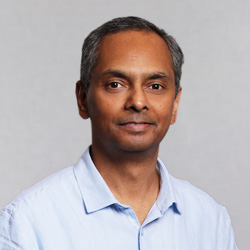
For health plan CIOs, cost pressure now centers on a single metric: medical loss ratio (MLR). As medical and pharmacy costs outpace premium growth, every unmanaged dollar flows straight into it. The pressure is already visible (see Exhibit 1). GLP-1s drove nearly half of the 2024 increase in commercial drug spend, and most large insurers reported higher MLRs through 2025, with Centene reaching 91.9%.
Sources: IFEBP/SHRM, 2025; Evernorth, 2025; KFF, 2026; Becker’s, 2026. Analysis: HFS Research, 2026
Health plans have responded with the levers they know best: utilization management, prior authorization, and care management. These decide what gets approved and paid, but they never reach the underlying risk: the chronic disease and specialty-therapy exposure that drives cost in the first place. The result is more administrative friction without a durable bend in trend, because the insight that could prevent the rising cost remains trapped in analytics dashboards and quarterly reviews, disconnected from the claims, care management, and member-outreach systems where intervention actually happens. The gap is not analytic capability; it is the absence of an operating layer that turns a risk signal into a triggered, owned, and measured action inside existing workflows.
Plans already hold the signals that flag a member heading toward a high-cost event. What they lack is the infrastructure to act on those signals, not after it is locked in.
This playbook introduces a Services-as-Software approach to turn those signals into timely action using existing systems and workflows without a large upfront transformation program. It enables three shifts:
Implementing population risk management lowers medical costs that affect MLR, reduces the operational burden of managing high-friction cost controls, and highlights the impact of each intervention, enabling health plans to invest in effective solutions and discontinue those that do not work.
Financial impact
Operational impact
Outcomes visibility
The opportunity cost of continuing to rely on reactive, transactional cost controls is increasingly unsustainable in a high-trend, margin-constrained environment.
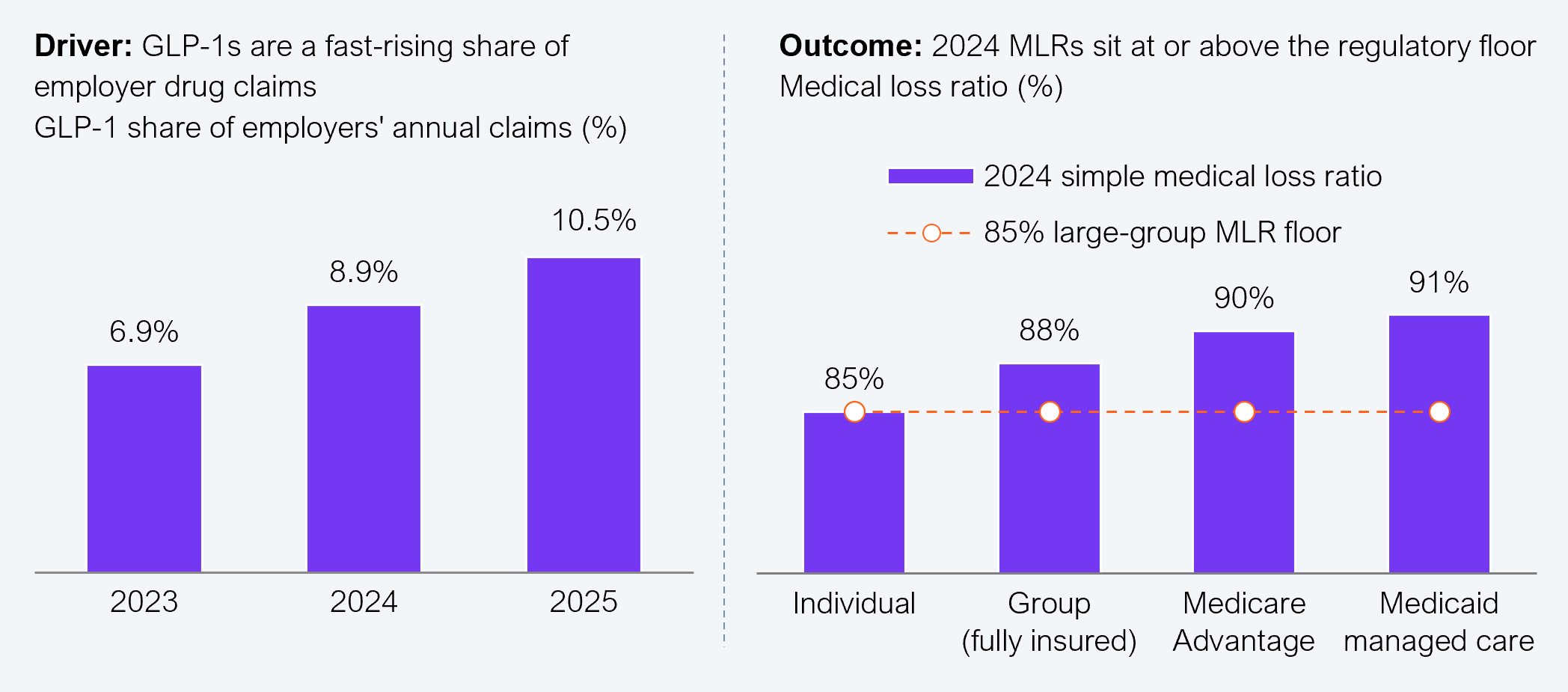
Rather than launching another transformation program or buying more standalone tools, health plans should operationalize population risk management as a service. This involves using AI to detect rising risk, trigger intervention, and measure the resulting financial outcomes in PMPM and MLR, all within the systems they already run (see Exhibit 2):
Source: HFS Research, 2026
This is where Services-as-Software can earn its place. Rather than relying on large transformation programs, it helps health plans operationalize AI for earlier risk detection, consistent intervention, and measurable financial outcomes. And because population risk management spans clinical, operational, and financial functions, it serves as a common operating model that aligns stronger alignment among business leaders, typically market presidents, line-of-business heads, and clinical, operations, and financial stakeholders. More importantly, the CIO’s job shifts from leading technology transformation to supporting business-led cost control strategies by enabling AI-driven risk detection, scalable intervention infrastructure, and telemetry-based outcome measurement.
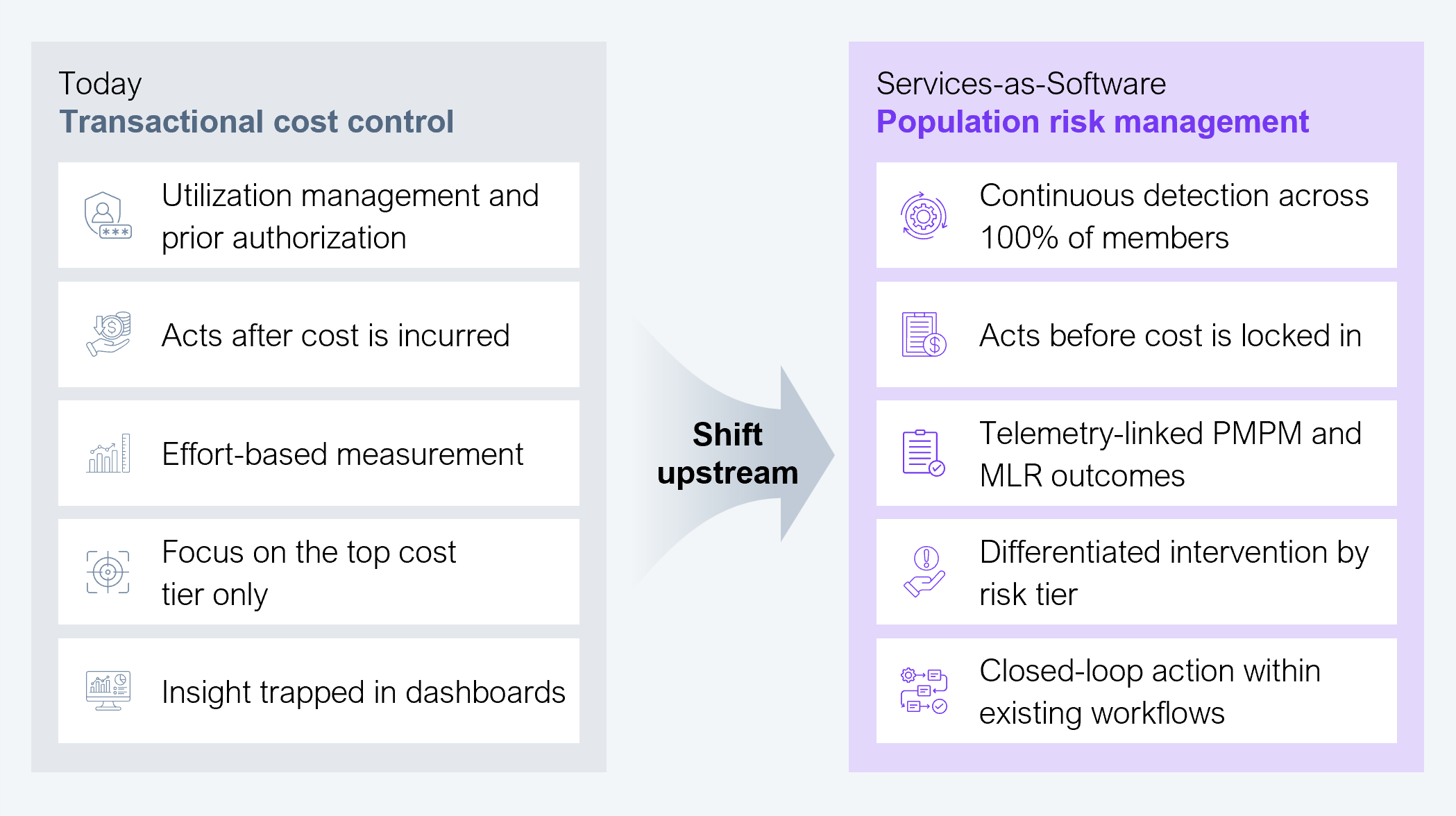
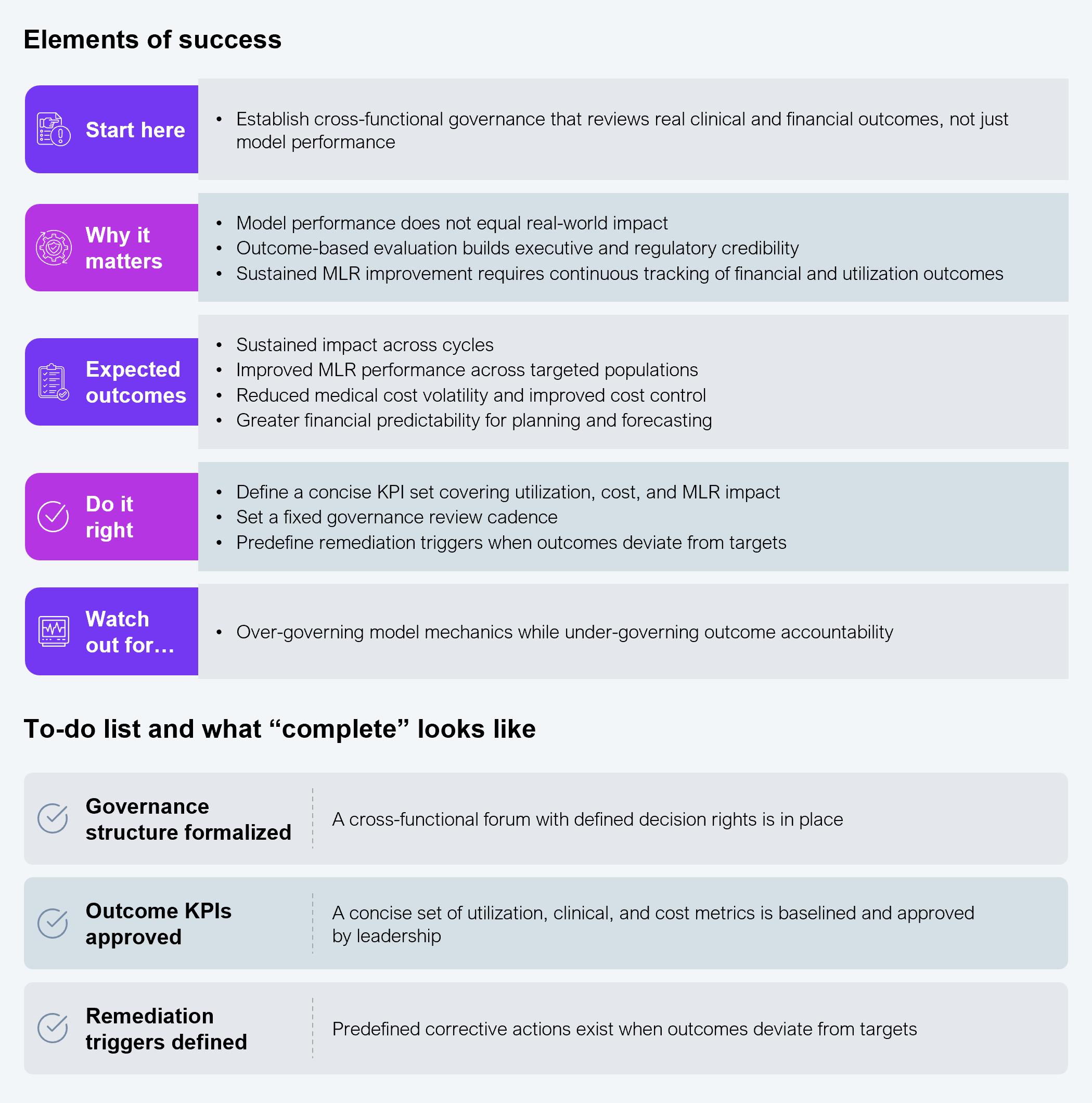
But technology is only the starting point. Models, dashboards, and risk scores alone do not deliver value. Real value is only fully realized through measurable financial outcomes, including PMPM cost reduction and improved MLR performance. The real shift is moving away from investing in standalone capabilities to operationalizing measurable financial and utilization impact. Because population risk management directly impacts cost, MLR, and regulatory compliance, the execution must be sequenced, practical, and aligned to business priorities (see Exhibit 3).
Source: HFS Research, 2026
When a new operating paradigm is being adopted, execution discipline matters more than ambition. The following sections underline the key tenets of each step in the playbook to ensure population risk management delivers measurable outcomes rather than remaining an analytical exercise.
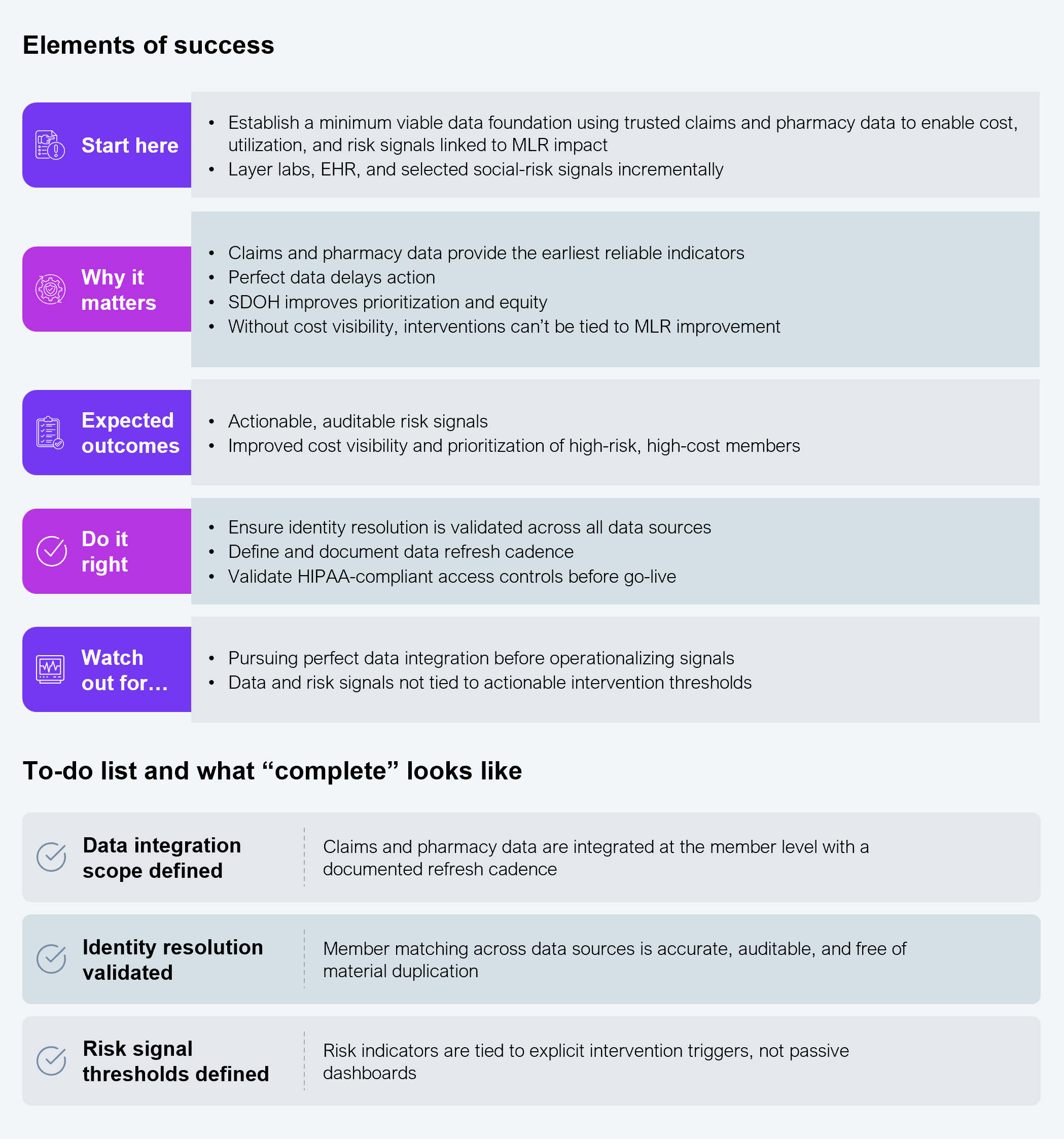
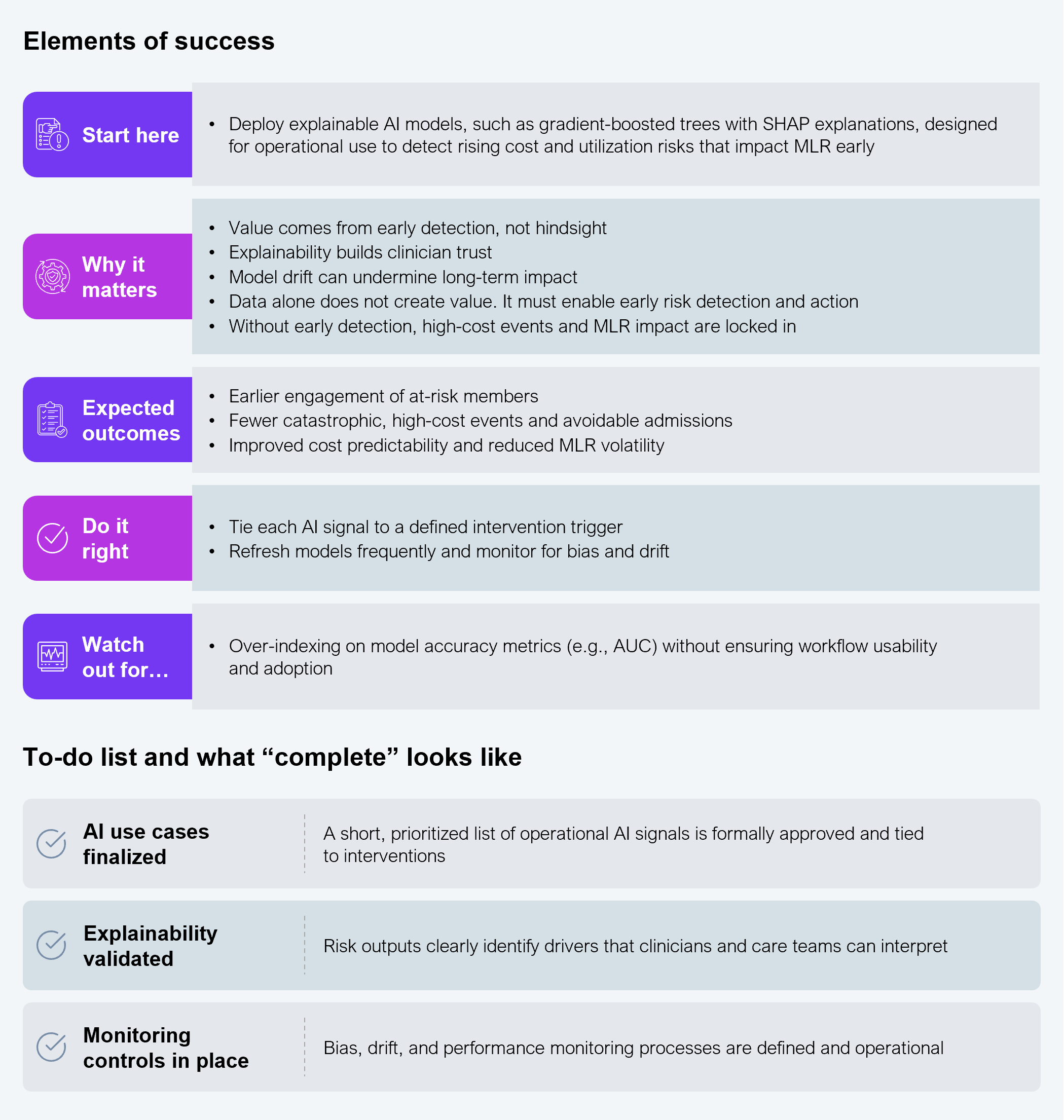
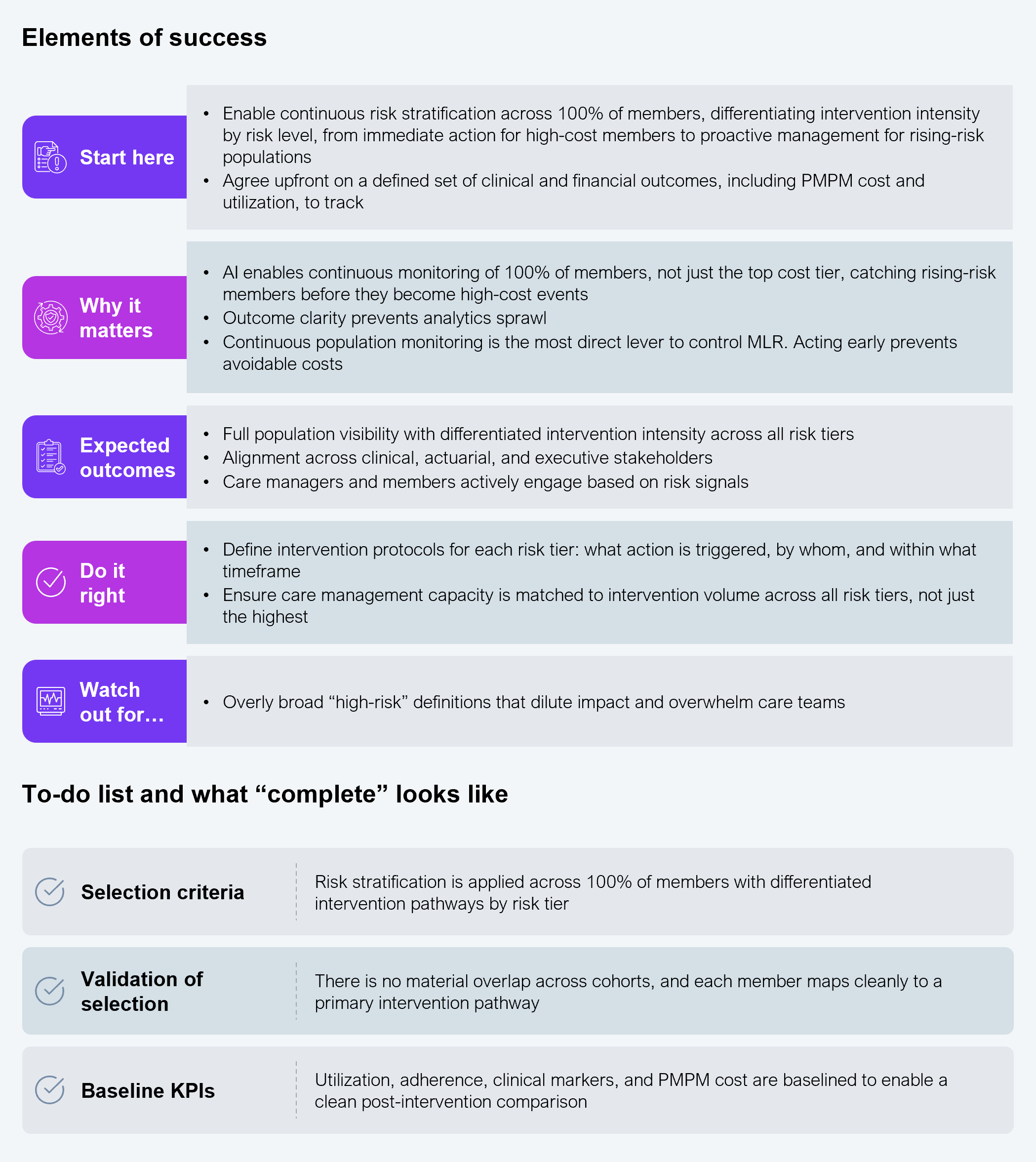
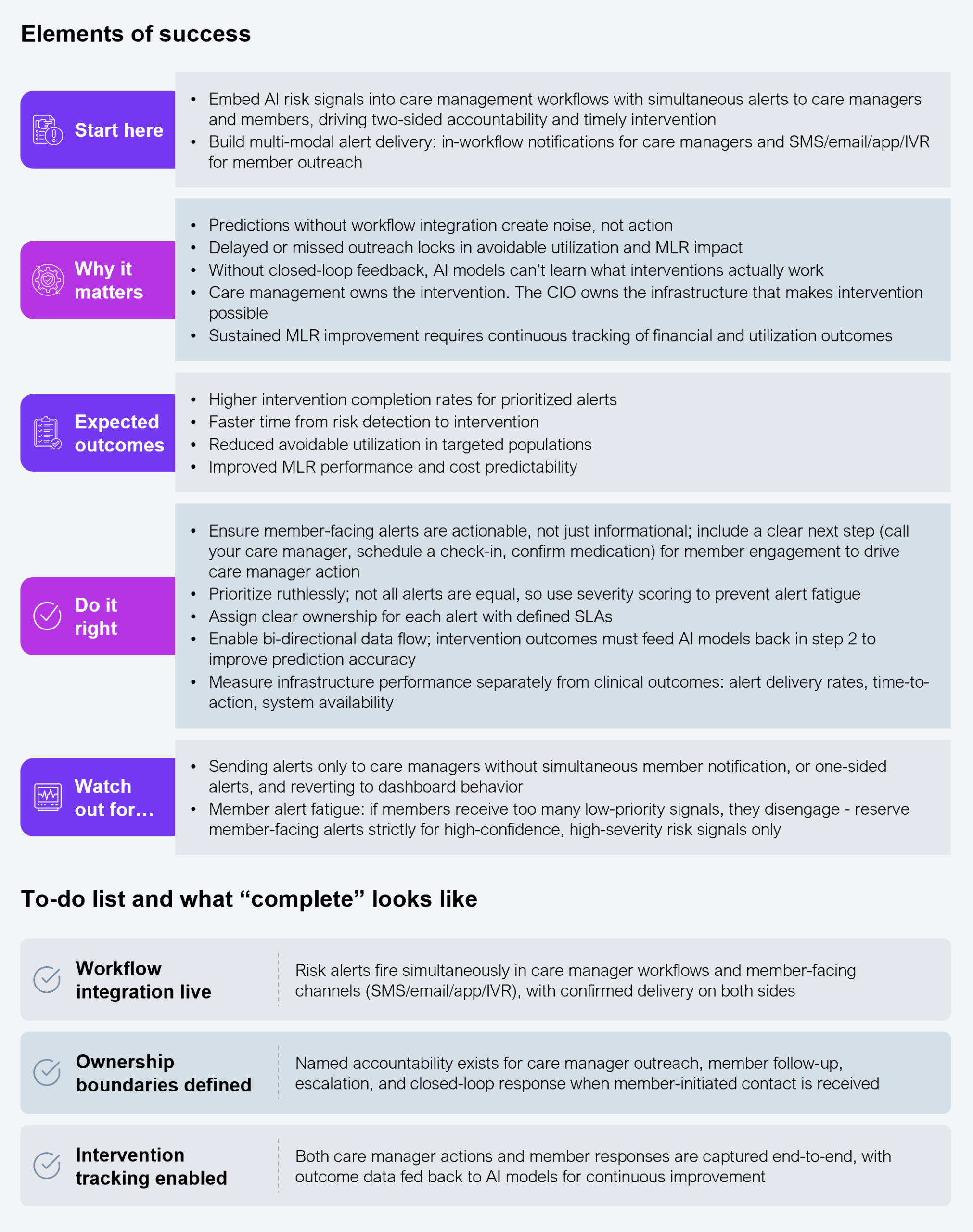
Health plan leaders must avoid analysis paralysis by adopting a least-resistant execution path focused on reducing cost and improving MLR outcomes. Initial data readiness and AI-driven risk detection must be completed within the first 8–12 weeks, immediately followed by rapid cohort prioritization and workflow integration (see Exhibit 4). Measurable improvements in PMPM cost, utilization, and MLR performance should be visible within one or two quarters. If material progress is not achieved within a year of execution, it must be reassessed.
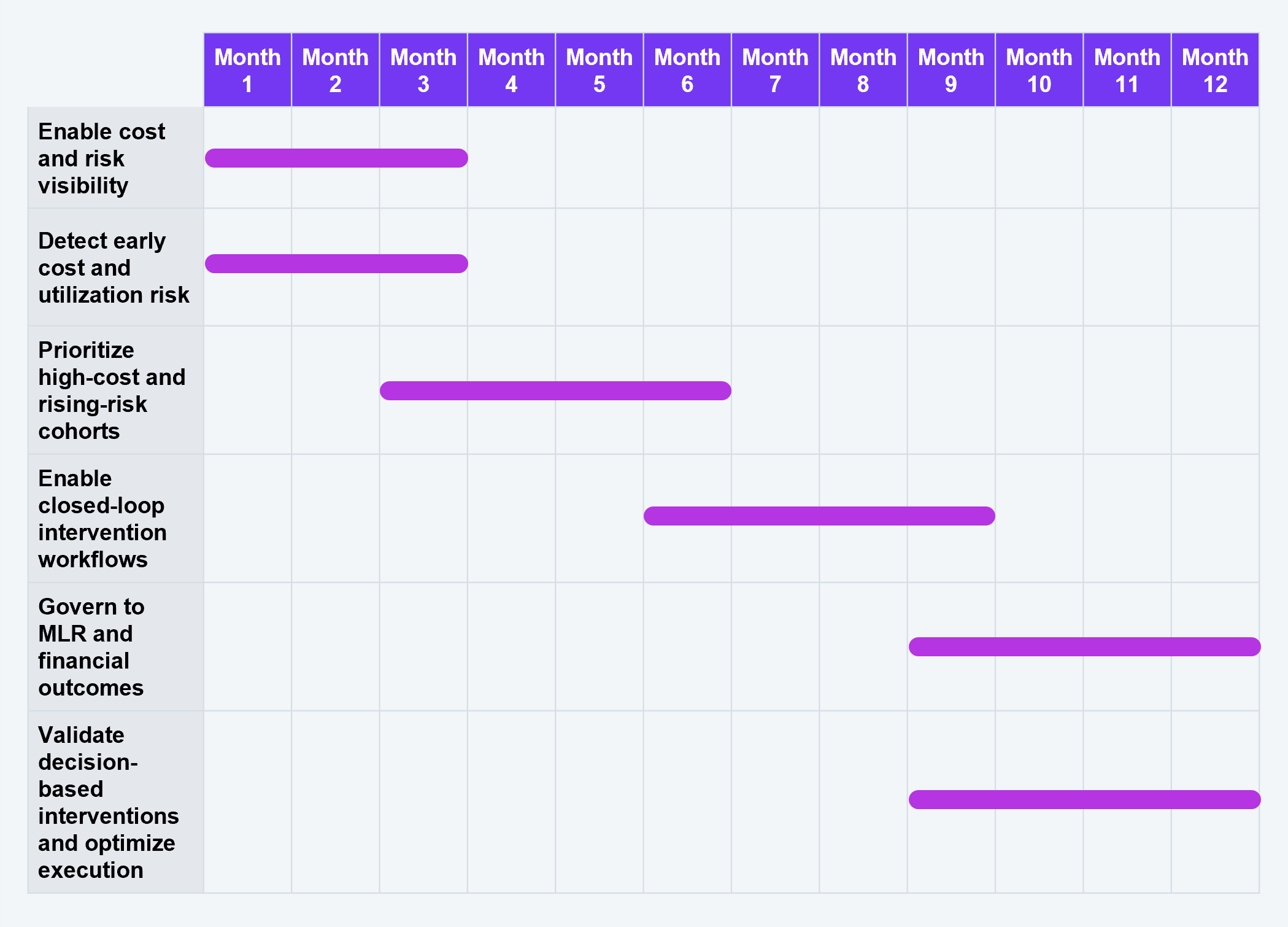
Source: HFS Research, 2026
As AI becomes embedded in population risk management, the biggest threats to sustained MLR improvement are behavioral, not technical. Once the platform works, three patterns quietly erode the gains:
None of these risks is about technology failing, but about leaders becoming comfortable. AI can flag the risk, but only disciplined execution and clear ownership convert detection into sustained MLR improvement.
Health plans have spent a decade automating the transactional layer: prior authorization, claims, documentation, and call centers. Those gains are real and now fully priced into the market. The next basis points of MLR performance will not come from automating more transactions, but from intervening before cost is incurred.
CIOs who shift AI investment from transaction automation to population-risk infrastructure, covering continuous detection, closed-loop intervention, and PMPM-linked governance, will convert AI into an MLR-defense asset. Those who keep scaling administrative automation will stabilize the cost of operations while medical costs continue to erode margins.
Check out our other perspectives
Register now for immediate access of HFS' research, data and forward looking trends.
Get StartedIf you don't have an account, Register here |
With the exception of our Horizons reports, most of our research is available for free on our website. Sign up for a free account and start realizing the power of insights now.
Our premium subscription gives enterprise clients access to our complete library of proprietary research, direct access to our industry analysts, and other benefits.
Contact us at [email protected] for more information on premium access.